維持性腹膜透析患者肺淤血與生活質量的關系
2017-07-05 12:54:51王加偉盧來順洪春燕王良玉唐小玲
山東醫藥 2017年22期
王加偉,盧來順,洪春燕,王良玉,唐小玲
(汕頭市中心醫院,廣東汕頭 515041)
維持性腹膜透析患者肺淤血與生活質量的關系
王加偉,盧來順,洪春燕,王良玉,唐小玲
(汕頭市中心醫院,廣東汕頭 515041)
目的 觀察維持性腹膜透析患者肺淤血及生活質量情況,并探討兩者的關系。方法 收集105例維持性腹膜透析患者的相關臨床資料,應用肺超聲顯示的B線數目評估肺淤血,采用簡明健康調查問卷(SF-36)評估生活質量,計算軀體健康總分(PCS)與精神健康總分(MCS)。采用Spearman相關分析B線數目與PCS、MCS的相關性。按PCS、MCS的中位數值將患者分為高PCS者與低PCS者、高MCS者與低MCS者,并比較兩者相關指標的差異,采用logistic回歸分析確定生活質量的獨立影響因素。結果 105例患者B線數目為4(0,17)條,存在肺淤血52例,PCS為52.8(44.8,59.8)分、MCS為54.5(46.8,60.8)分。B線數目與PCS、MCS呈負相關(r分別為-0.589、-0.464,P均<0.01)。與高PCS者相比,低PCS者B線數目、血B型尿鈉肽、年齡、糖尿病腎病比例和心腦血管疾病史比例高(P均<0.05),血紅蛋白、血白蛋白低(P均<0.01)。與高MCS者相比,低MCS者B線數目、血B型尿鈉肽高(P均<0.01),血紅蛋白、血白蛋白低(P均<0.01)。多因素分析結果顯示,B線數目、血紅蛋白水平、年齡及心腦血管疾病史是PCS的獨立影響因素(P均<0.05),但僅前兩者是MCS的獨立影響因素(P均<0.05)。結論 維持性腹膜透析患者肺淤血發生率較高且生活質量較低。肺淤血可能是患者生活質量下降的重要原因。
腹膜透析;肺淤血;生活質量;肺超聲;慢性腎功能衰竭
終末期腎臟病患者盡管可接受維持性透析治療,但其生活質量仍顯著低于普通人群。已有研究發現,維持性透析患者生活質量下降的危險因素有微炎癥、營養不良、殘余腎功能等,但因研究人群、研究方法、文化、經濟等不同而缺乏一致性結論[1~3]。維持性透析患者水鈉潴留可引起容量超負荷,心肌肥厚、冠狀動脈硬化、瓣膜病變、心律失常等可引起心臟收縮和舒張功能下降,兩者綜合作用可導致肺淤血的發生[4]。肺淤血可導致患者運動功能及生活質量下降。但目前有關肺淤血對維持性透析患者生活質量影響的研究較少[5~7]。因此,本研究觀察了維持性腹膜透析患者肺淤血、生活質量情況,并探討兩者的關系,為改善該人群的生活質量提供依據。
1 資料與方法
1.1 臨床資料 選擇2016年2~10月在汕頭市中心醫院腹膜透析中心治療的105例維持性腹膜透析患者,其中男60例、女45例;年齡(52.1±12.3)歲;BMI≥24 kg/m2者31例;已婚96例;有吸煙史者27例;存在心腦血管疾病史者25例;文化程度在小學及以下者55例,小學以上者50例;醫療報銷比例80%以上者37例。慢性腎功能衰竭病因為慢性腎炎49例、糖尿病腎病35例、其他病因或病因不明者21例。患者殘余尿量為300(50,700)mL/d,尿素清除指數為2.00±0.55。腹膜透析齡15.0(3.0,36.5)個月,劑量為8 L/d者93例、6 L/d者7例、10 L/d者5例。有92例患者行腹膜平衡試驗及透析充分性檢查,其中腹膜轉運類型為高轉運者19例、高平均轉運者35例、低平均轉運者33例、低轉運者5例。入選標準:年齡≥18歲;接受持續不臥床腹膜透析≥3個月;病情穩定;同意參與本研究并簽署知情同意書。排除標準:近3個月內出現急性心腦血管事件、創傷及手術等嚴重疾病;近1個月內發生腹膜炎或其他嚴重感染;存在除心力衰竭以外的其他臟器衰竭;需治療的惡性腫瘤;嚴重認知功能障礙;近1個月內服用抗焦慮抑郁藥物超過1周;長期服用可能導致或加重抑郁的藥物;肺間質纖維化、肺栓塞、肺切除、胸廓畸形或顯著肥胖等影響肺超聲檢查的情況;量表或相關臨床數據缺失影響分析者。本研究經中山大學附屬汕頭醫院倫理委員會審查、批準。
1.2 肺淤血觀察方法 應用荷蘭Philips IU22超聲儀配凸形探頭(頻率2~5 MHz),采用指南推薦的“28點掃描技術”[8~10]。患者取平臥位或近平臥位,充分暴露前胸壁及兩側胸壁,平靜呼吸。選擇二維超聲成像模式,探頭垂直胸壁,縱向掃描各肋間隙。以胸骨旁線、鎖骨中線、腋前線、腋中線與各肋間隙(右胸第2~5與左胸第2~4肋間隙)的28個交點作為檢查點,記錄各點的B線數目后求出總和。B線呈現為一種激光樣、垂直的、從胸膜線延伸到屏幕底部的無衰減的高回聲偽像。依據B線數目將肺淤血分4級:≤5條為無、6~15條為輕度、16~30條為中度、>30條為重度[8]。
1.3 生活質量評估方法 應用簡明健康調查問卷(SF-36)評估患者生活質量[11],計算軀體健康總分(PCS)與精神健康總分(MCS)。PCS包括軀體功能、軀體角色、軀體疼痛、一般健康狀況評分,MCS包括精力、社會功能、情緒角色和精神健康評分。

2 結果
2.1 維持性腹膜透析患者肺淤血情況 維持性腹膜透析患者B線數目為4(0,17)條,存在肺淤血52例,其中中重度肺淤血34例。52例肺淤血患者中有明顯下肢水腫、氣促癥狀者28例。
2.2 維持性腹膜透析患者的生活質量情況 維持性腹膜透析患者PCS為52.8(44.8,59.8)分,MCS為54.5(46.8,60.8)分,其中軀體功能評分為80.0(70.0,85.0)分,軀體角色評分為25.0(0.0,25.0)分,軀體疼痛評分為74.0(61.0,84.0)分,一般健康狀況評分為42.0(30.0,50.0)分,精力評分為45.0(40.0,55.0)分,社會功能評分為62.5(50.0,75.0)分,情緒角色評分為33.3(33.3,66.7)分,精神健康評分為76.0(60.0,80.0)分。
2.3 維持性腹膜透析患者肺淤血與生活質量的關系 維持性腹膜透析患者B線數目與PCS、MCS呈負相關(r分別為-0.589、-0.464,P均<0.01)。
2.3.1 單因素分析結果 見表1。
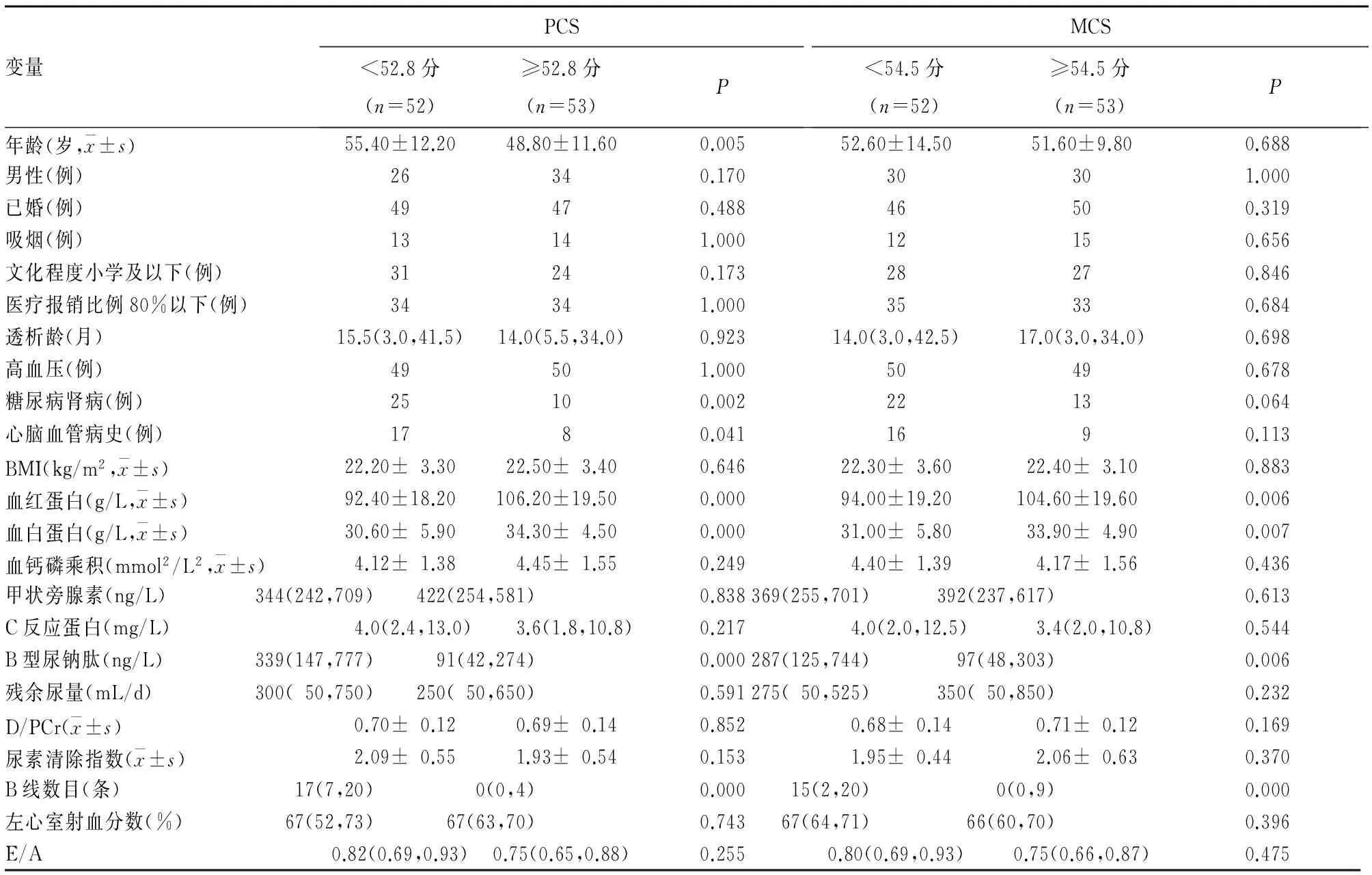
表1 維持性腹膜透析患者生活質量影響因素的單因素分析結果
注:D/PCr為腹膜平衡試驗中4 h透出液與血液中肌酐濃度比值;E/A為組織多普勒測定的舒張早期與舒張晚期二尖瓣最大血流速度的比值。
2.3.2 多因素logistic回歸分析結果 見表2、3。

表2 維持性腹膜透析患者PCS下降的多因素logistic回歸分析結果
注:模型經糖尿病腎病比例、血B型尿鈉肽、血白蛋白校正。

表3 維持性腹膜透析患者MCS下降的多因素logistic回歸分析結果
注:模型經糖尿病腎病比例、血B型尿鈉肽、血白蛋白校正。
3 討論
隨著社會-心理-生物醫學模式的不斷發展,生活質量已成為患者健康綜合評估的重要部分。了解維持性腹膜透析患者的生活質量及其影響因素,幫助其提高、保持生活質量是終末期腎臟病治療的一項重要任務。肺超聲不僅對胸腔積液、胸膜病變有良好的診斷價值,而且還能很好地檢測出肺淤血、肺實變等病變[8~10]。2012年國際肺超聲聯絡委員會及2015年歐洲心臟病學會均在指南中推薦肺超聲作為評估心力衰竭者肺淤血的一線檢查[9,12]。肺超聲用于評估腎臟病人群肺淤血的應用也日漸增多[5,6,9,13,14]。SF-36評價生活質量的可靠性也已在維持性透析人群中得到充分驗證,并在臨床實踐及研究中被廣泛采用[1~3,11]。因此,本研究采用肺超聲對患者的肺淤血進行評估,應用SF-36評價患者生活質量。本研究105例腹膜透析患者中52例存在肺淤血,且34例為中重度肺淤血。既往有研究[6,13]發現,腹膜透析患者肺淤血中中重度肺淤血發生率在40%左右。本研究患者的生活質量總體上較低,結果亦與國內外研究[2~3]相近。可見,腹膜透析患者肺淤血發生率較高而生活質量較低。
本研究進一步分析發現,B線數目與血紅蛋白水平是PCS和MCS的獨立影響因素。B線數目的增加意味著肺間質水分的增多(肺淤血),進一步提示機體可能存在容量超負荷和(或)心臟功能下降。而容量超負荷已被證實可導致血壓控制不良、增加心臟前后負荷、促進血管硬化和心肌重構,導致活動耐量降低及心力衰竭進展,增加心血管疾病發生率[4,14,15],從而可能導致患者的PCS和MCS下降。Enia等[5]研究亦發現,肺超聲B線數目是腹膜透析患者軀體功能的獨立影響因素。貧血也可能通過降低血液的攜氧功能,進而降低心臟及中樞神經系統的機能,從而影響患者的軀體功能及精神健康[1,16]。與之前研究[1]結果類似,腹膜透析患者年齡的增長伴隨軀體功能的下降,但未觀察到高齡導致腹膜透析患者精神健康的下降;不同的是,之前研究[1]認為心腦血管疾病史是腹膜透析患者PCS與MCS的獨立影響因素[1],但本研究心腦血管疾病史未能預測MCS的下降,原因可能與研究樣本量較小、人群差異或者存在其他混雜因素有關。
本研究中左心室射血分數與生活質量評分無顯著相關性;血B型尿鈉肽只在單因素分析中顯示與生活質量評分存在顯著相關性。究其原因,可能是左心室射血分數只反映了左心收縮功能,而超過一半的腹膜透析患者表現為射血分數正常的心力衰竭[17];B型尿鈉肽雖反映容量負荷,但腎衰竭時其腎臟清除減少從而影響其診斷效能[18]。本研究未發現文化程度、透析充分性、糖尿病腎病與低白蛋白血癥等是生活質量下降的獨立危險因素。目前有關這些因素對腹膜透析患者生活質量的影響尚有爭論[1~3,19~21],需要更多高質量的研究來進一步確定。
本研究存在的缺陷:本研究是一個單中心研究,且樣本量仍偏小,其結論是否能推廣至其他腹膜透析人群尚有待驗證;由于橫斷面研究的局限性,需要進一步確認肺淤血與生活質量的因果關系;生活質量受多種主觀及客觀因素影響,一些本研究未涉及的因素如種族、宗教信仰、人格特征、經濟收入、社會支持等還有待探討。
[1] dos Santos Grincenkov FR, Fernandes N, Chaoubah A, et al. Longitudinal changes in health-related quality of life scores in Brazilian incident peritoneal dialysis patients (BRAZPD): socio-economic status not a barrier[J]. Perit Dial Int, 2013,33(6):687-696.
[2] 劉瑩,韓慶烽,唐雯,等.腹膜透析患者生活質量的相關影響因素分析[J].中國血液凈化,2016,15(6):367-370.
[3] Park HC, Lee H, Lee JP, et al. Lower residual renal function is a risk factor for depression and impaired health-related quality of life in Korean peritoneal dialysis patients[J]. J Korean Med Sci, 2012,27(1):64-71.
[4] Zoccali C, Tripepi R, Torino C, et al. Lung congestion as a risk factor in end-stage renal disease[J]. Blood Purify, 2013,36(3-4):184-191.
[5] Enia G, Torino C, Panuccio V, et al. Asymptomatic pulmonary congestion and physical functioning in hemodialysis patients[J]. Clin J Am Soc Nephrol, 2013,8(8):1343-1348.
[6] Enia G, Tripepi R, Panuccio V, et al. Pulmonary congestion and physical functioning in peritoneal dialysis patients[J]. Perit Dial Int, 2012,32(5):531-536.
[7] Yoon HE, Kwon YJ, Song HC, et al. Overhydration negatively affects quality of life in peritoneal dialysis patients: evidence from a prospective observational study[J]. Int J Med Sci, 2016,13(9):686-695.
[8] Picano E, Pellikka PA. Ultrasound of extravascular lung water:a new standard for pulmonary congestion[J]. Eur Heart J, 2016,37(27):2097-2104.
[9] Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence-based recommendations for point-of-care lung ultrasound[J]. Intensive Care Med, 2012,38(4):577-591.
[10] Jambrik Z, Monti S, Coppola V, et al. Usefulness of ultrasound lung comets as a nonradiologic sign of extravascular lung water[J]. Am J Cardiol, 2004,93(10):1265-1270.
[11] Moreno F, López Gomez JM, Sanz-Guajardo D, et al. Quality of life in dialysis patients. A Spanish multicenter study. Spanish Cooperative Renal Patients Quality of Life Study Group[J]. Nephrol Dial Transplant, 1996,11(Suppl 2):125-129.
[12] Mebazaa A, Yilmaz MB, Levy P, et al. Recommendations management on pre-hospital and hospital of acute heart failure: a consensus paper of the Heart Failure Association of the European Society of Cardiology, the European Society of Emergency Medicine and the Society of Academic Emergency Medicine[J]. Eur J Heart Fail, 2015,17(6):544-558.
[13] Panuccio V, Enia G, Tripepi R, et al. Chest ultrasound and hidden lung congestion in peritoneal dialysis patients[J]. Nephrol Dial Transplant, 2012,27(9):3601-3605.
[14] Zoccali C, Torino C, Tripepi R, et al. Pulmonary congestion predicts cardiac events and mortality in ESRD[J]. J Am Soc Nephrol, 2013,24(4):639-646.
[15] Essig M, Escoubet B, de Zuttere D, et al. Cardiovascular remodelling and extracellular fluid excess in early stages of chronic kidney disease[J]. Nephrol Dial Transplant, 2008,23(1):239-248.
[16] Liu H, Yao Y, Cao Y, et al. Anemia management trends in patients on peritoneal dialysis in the past 10 years[J]. Int J Clin Exp Med, 2015,8(10):18050-18057.
[17] Wang AY, Wang M, Lam CW, et al. Heart failure with preserved or reduced ejection fraction in patients treated with peritoneal dialysis[J]. Am J Kidney Dis, 2013,61(6):975-983.
[18] Wang AY, Lai KN. Use of cardiac biomarkers in end-stage renal disease[J]. J Am Soc Nephrol, 2008,19(9):1643-1652.
[19] Yang F, Griva K, Lau T, et al. Health-related quality of life of Asian patients with end-stage renal disease (ESRD) in Singapore[J]. Qual Life Res, 2015,24(9):2163-2171.
[20] Li J, Wu X, Lin J, et al. Type D personality, illness perception, social support and quality of life in continuous ambulatory peritoneal dialysis patients[J]. Psychol Health Med, 2017,22(2):196-204.
[21] Chen JB, Lam KK, Su YJ, et al. Relationship between Kt/V urea-based dialysis adequacy and nutritional status and their effect on the components of the quality of life in incident peritoneal dialysis patients[J]. BMC Nephrol, 2012,14(13):39.
Relationship between pulmonary congestion and quality of life in maintenance peritoneal dialysis patients
WANGJiawei,LULaishun,HONGChunyan,WANGLianyu,TANGXiaoling
(ShantouCentralHospital,Shantou515041,China)
Objective To observe the pulmonary congestion (PC) and quality of life (QOL) in maintenance peritoneal dialysis (MPD) patients and to investigate the relationship between them. Methods We collected the clinical data of 105 MPD patients, evaluated PC with B-line number on pulmonary ultrasonography, evaluated QOL by concise health questionnaire (SF-36), and calculated the physical health score (PCS) and mental health score (MCS). The association between B line number and PCS, MCS was examined by Spearman correlation analysis. Patients were respectively divided into two groups according to the median of PCS and MCS. Demographic data and clinical parameters were compared between the two groups, and then multivariate binary logistic regression analysis was applied to determine the independent risk factors for QOL. Results A total of 105 MPD patients were included. Median B line number was 4 (0,17). PC was detected in 52 cases, PCS was 52.8 (44.8, 59.8) points, and MCS was 54.5 (46.8, 60.8) points. B line number was negatively correlated with PCS and MCS (r=-0.589, -0.464, bothP<0.01). Compared with patients with high PCS, B lines number, serum B-type natriuretic peptide, average age, proportion of diabetic kidney disease and proportion of previous cardiocerebrovascular events were higher (P<0.05), while hemoglobin and serum albumin were lower in patients with low PCS (bothP<0.01). Compared with patients with high MCS, B line number and serum B-type natriuretic peptide were higher (bothP<0.01), but hemoglobin and serum albumin were lower in patients with low MCS (bothP<0.01). Multivariate analysis showed that B line number, hemoglobin, age, and previous cardiocerebrovascular events were independent risk factors for PCS (allP<0.01), however, only B line number and hemoglobin were independent risk factors for MCS (bothP<0.05). Conclusion MPD patients have high prevalence of PC and low level of QOL, and PC may be an important reason for the decline of QOL in these patients.
peritoneal dialysis; pulmonary congestion; quality of life; lung ultrasonography; chronic renal failure
廣東省醫學科研基金項目(B2016115)。
王加偉(1983-),男,碩士,主治醫師,主要從事慢性腎臟病的容量控制研究。E-mail: jiaweiwang1983@gmail.com
唐小玲(1962-),女,本科,主任醫師,主要從事慢性腎臟病的微炎癥研究。E-mail: gdsttxl@163.com
10.3969/j.issn.1002-266X.2017.22.006
R459.5;R445.1
A
1002-266X(2017)22-0019-04
2017-01-06)
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
中學生數理化·八年級物理人教版(2021年12期)2021-12-31 03:23:08
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
中學生數理化·中考版(2020年10期)2020-11-27 01:59:48
科技傳播(2019年22期)2020-01-14 03:06:54
中國生殖健康(2019年2期)2019-08-23 08:12:08
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
少年博覽·小學高年級(2016年12期)2017-01-16 12:48:35
特別文摘(2016年19期)2016-10-24 18:38:15
37°女人(2016年5期)2016-05-06 19:44:06
