前列地爾聯合丹參川芎嗪治療腔隙性腦梗死眩暈的臨床效果
2017-09-20 02:28:53苗新亞
中國當代醫藥 2017年23期
苗新亞
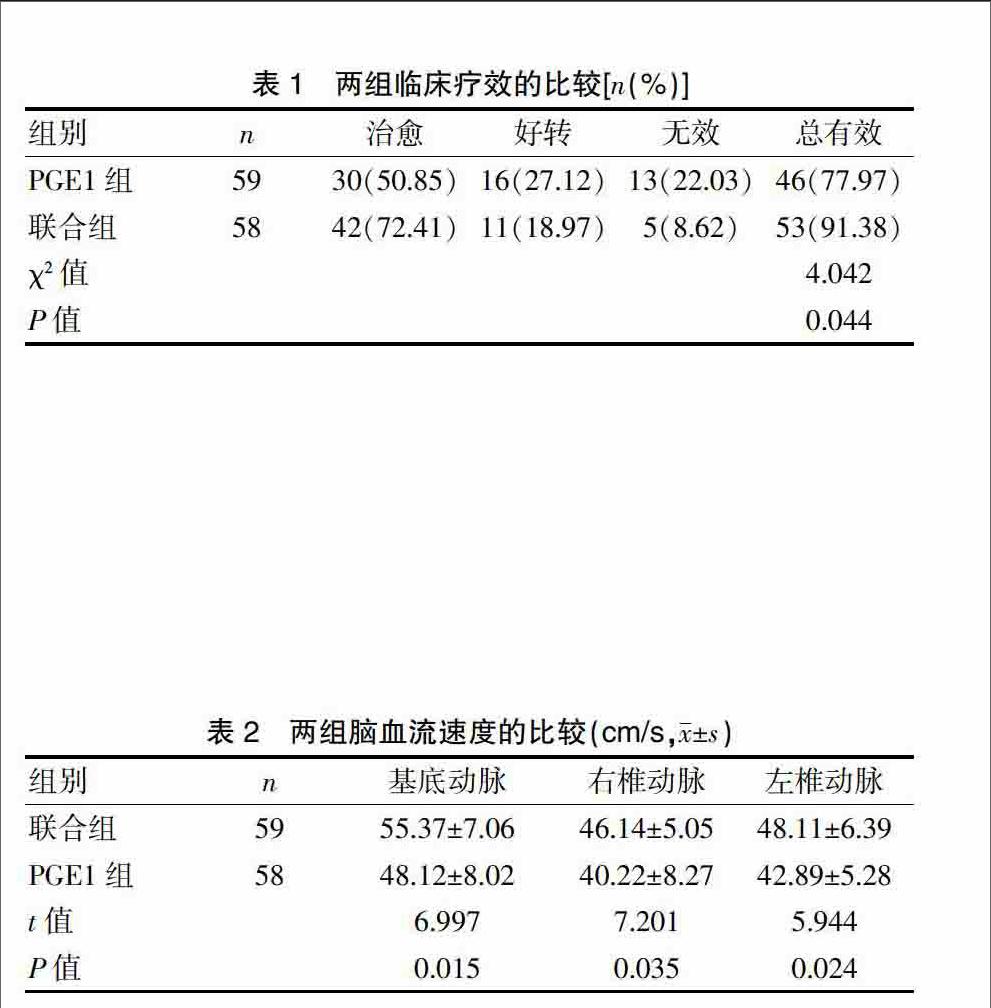
[摘要]目的 研究中藥針劑丹參川芎嗪聯合前列地爾(PGE1)治療腔隙性腦梗死(LI)眩暈的效果。方法 選擇我院2015年8月~2017年4月治療的117例LI患者,隨機分為PGE1組(59例)和聯合組(58例)。聯合組使用中藥針劑丹參川芎嗪聯合PGE1治療,PGE1組采用PGE1治療。對比兩組的療效以及腦血流情況,包括基底動脈、右椎動脈及左椎動脈血流。結果 聯合組的總有效率為91.38%,高于PGE1組的77.97%,差異有統計學意義(P<0.05)。聯合組的腦血流速度顯著高于PGE1組,差異有統計學意義(P<0.05)。結論 聯合中藥復方制劑丹參川芎嗪與PGE1治療LI眩暈的療效確切。
[關鍵詞]腦梗死;川芎嗪;前列地爾
[中圖分類號] R43.33 [文獻標識碼] A [文章編號] 1674-4721(2017)08(b)-0133-03
Clinical effect of Alprostadil combined with Salviaemiltiorrhizae and Ligustrazine in the treatment of vertigo due to lacunar infarction
MIAO Xin-ya
Department of Encephalopathy,Traditional Chinese Medicine Hospital of Pizhou City in Jiangsu Province,Pizhou 221300,China
[Abstract]Objective To study the effect of injection of Salviaemiltiorrhizae and Ligustrazine combined with Alprostadil (PGE1) on treating vertigo due to lacunar infarction (LI).Methods From August 2015 to April 2017,117 LI patients treated in our hospital were selected and randomly divided into the PGE1 group (n=59) and the combination group (n=58).In the combination group,injection of Salviaemiltiorrhizae and Ligustrazine was selected for treatment,while in the PGE1 group,PGE1 was adopted.The effect on treating vertigo and cerebral blood flow including basilar artery,right vertebral artery,and left vertebral artery blood flow were compared in the two groups.Results The effective rate in the combined group was 91.38%,which was higher than that in the PGE1 group accounting for 77.97%,with statistical difference (P<0.05).The cerebral blood flow velocity in the combined group was significantly faster than that in the PGE1 group,with significant difference (P<0.05).Conclusion The combination of traditional Chinese herbal medicine compound preparation of Salviaemiltiorrhizae and Ligustrazine combined with PGE1 can obtain a definite effect on treating vertigo due to LI.
[Key words]Cerebral infarction;Ligustrazine;Alprostadil
腔隙性腦梗死(lacunar infarction,LI)軟化病灶位于腦深部核團、白質或腦干,閉塞穿支動脈以終末動脈為主,直徑為40~50 μm,微梗塞腔隙徑線多≤15 mm,側支循環形成難度大,LI組織缺氧缺血、Na+-K+-ATP酶異常、細胞代謝功能紊亂,容易發生毒性水腫,進而導致腦組織局限性壞死、液化,吞噬細胞可移走壞死及液化的腦組織,發展為腦軟化。糖尿病、肥胖癥、高血壓、腦部前支動脈異常出血均為LI發生風險信號。多發性LI可對腦部神經功能產生影響,引起反應遲鈍、眩暈、頭痛頭暈、記憶力減退等癥狀,甚至可能造成智力衰退或癡呆[1]。治療LI時應注意抗凝、擴張血管及增加大腦血液灌注,改善神經功能及預防復發。眩暈是LI常見自覺癥狀,本研究旨在分析前列地爾(PGE1)聯合丹參川芎嗪治療LI眩暈的效果,現報道如下。
1資料與方法
1.1一般資料
收集2015年8月~2017年4月在我院就診的117例LI患者的資料,均主訴間斷眩暈或連續眩暈,呈搖擺感、晃動感或旋轉性,頭頸位發生變化時可誘發或加重眩暈,可出現復視、眼蒙及眼花等視覺癥狀,Romberg征陽性、站立不穩或步態不穩、眼球震顫、飲水嗆咳、情感淡漠、精神抑郁、視野缺損、視物模糊,合并吞咽障礙、吐詞不清、口眼歪斜、言語不利、惡心嘔吐、頭痛頭暈、記憶力或理解力變化、肢體麻木無力、耳鳴、昏厥、猝倒等,經頭顱DWI、MRA或CT確診[2-3]。所有入選患者均知情同意,本研究經我院醫學倫理委員會批準。排除對川芎嗪、丹參、PGE1成分過敏或抵抗,顱內出血或出血傾向,SBP/DBP>200 mmHg/110 mmHg,伴有腦腫瘤、Moyamoya病、囊蟲病、腦部感染者。將入選患者隨機分為PGE1組(59例)和聯合組(58例)。PGE1組中,男35例,女24例;年齡34~89歲,平均(66.9±5.2)歲;梗死部位:腦干15例,頂葉4例,丘腦12例,尾狀核6例,顳葉4例,側腦室旁5例,內外囊11例,小腦2例;梗死灶徑線為3~17 mm,平均(10.4±3.7)mm;LI眩暈誘因:氣候變化10例,飲酒17例,勞累或用力過度21例,情緒波動8例,其他3例。聯合組中,男33例,女25例;年齡35~88歲,平均(66.2±5.7)歲;梗死部位:腦干14例,頂葉3例,丘腦13例,尾狀核7例,顳葉2例,側腦室旁4例,內外囊12例,小腦3例;梗死灶徑線為2~19 mm,平均(10.1±3.2)mm;LI眩暈誘因:氣候變化9例,飲酒16例,勞累或用力過度20例,情緒波動9例,其他4例。兩組的性別、年齡、梗死部位、誘因等一般資料比較,差異無統計學意義(P>0.05),具有可比性。endprint