椎管內腸源性囊腫
2017-11-21 11:46:23韓彤
中國現代神經疾病雜志 2017年7期
關鍵詞:信號
.臨床醫學圖像.
椎管內腸源性囊腫
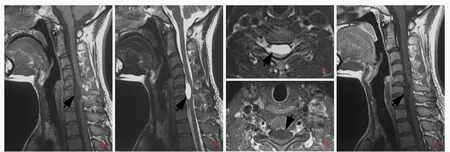
圖1 男性患者,29歲,因肩部疼痛1個月就診.頸椎MRI顯示椎管內髓外囊性占位征象.予頸椎椎管內占位性病變探查術.術后病理證實腸源性囊腫 1a 矢狀位T1WI顯示,C5~7水平椎管內髓外囊性信號影,長軸與脊髓平行,呈低信號,強度高于腦脊液(箭頭所示)1b 矢狀位T2WI顯示,病變呈均勻高信號,可見"脊髓嵌入征"(箭頭所示)1c 橫斷面T2WI顯示,病變位于脊髓腹側(箭頭所示)1d 橫斷面增強T1WI顯示病灶無強化(箭頭所示)1e 矢狀位增強T1WI顯示病變無強化(箭頭所示)Figure 1 A 29 ?year?old male was admitted to our hospital to investigate one month history of shoulder pain.MRI showed an intradural extramedullary occupied lesion located in cervical spinal canal. Then an exploratory craniotomy was performed and postoperative pathological diagnosis was intraspinal enterogenous cyst. Sagittal T1WI indicated an intradural extramedullary cystic hypointense lesion which intensity was higher than CSF located in the ventral subdural space through C5-7level.The long axis of lesion was parallel with the spine(arrow indicates,Panel 1a). Sagittal T2WI showed a subdural hyperintensity lesion with"spinal cord embedded syndrome"(arrow indicates,Panel 1b).Axial T2WI demonstrated a cystic hyperintensity appearing located in the ventral subdural space of spine cord and spine cord was compressed backwards obviously(arrow indicates,Panel 1c).Axial enhancement T1WI showed no enhancement within the lesion(arrow indicates,Panel 1d).Sagittal enhancement T1WI showed no enhancement within the lesion(arrow indicates,Panel 1e).
腸源性囊腫是臨床少見的內胚層發育障礙相關囊性病變,發病機制不清,多認為是胚胎發育第3周神經管與原腸分離障礙,殘留前腸或呼吸芽等內胚層組織與脊索結合演變而來.好發于青少年,男女比例為3∶2,多數發生于前中線處,以頸髓和上胸髓腹側多見,腰骶髓少見,常伴先天性脊柱畸形(如脊柱裂、蝴蝶椎、半椎體、皮膚瘺等)、腸管移位、消化道憩室,少數發生于顱后窩、橋前池、腦橋小腦角等.臨床癥狀與發生部位有關,主要為壓迫癥狀和囊液滲漏導致的刺激癥狀,表現為囊腫所在部位神經根性疼痛,伴運動障礙.CT呈椎管內髓外圓形或卵圓形水樣均勻低密度影,脊髓受壓變扁.MRI顯示病變邊緣光滑,長軸與脊髓平行,囊壁菲薄,厚度均勻;T1WI呈等或高于腦脊液信號(圖1a),若囊液內含有較多蛋白質或陳舊性出血,則呈等或高信號;T2WI呈等或低于腦脊液信號,脊髓明顯受壓變形,部分可于橫斷面或矢狀位見囊腫嵌入髓內,稱"脊髓嵌入征"(圖1b,1c),少數甚至可見囊腫包埋于髓內;增強掃描病變無明顯強化(圖1d,1e),少數囊壁呈線樣強化,多與假性鱗狀上皮化生或炎癥反應相關.不典型腸源性囊腫應注意與囊性神經鞘瘤和(或)神經纖維瘤、脊膜瘤、表皮樣囊腫、皮樣囊腫、畸胎瘤、脂肪瘤、蛛網膜囊腫、脊髓血管網織細胞瘤等髓外椎管內疾病相鑒別.
(天津市環湖醫院神經放射科韓彤供稿)
Intraspinal enterogenous cyst
HAN Tong
Department of Neuroradiology,Tianjin Huanhu Hospital,Tianjin 300350,China(Email:mrbold@163.com)
10.3969/j.issn.1672?6731.2017.07.013
猜你喜歡
鴨綠江(2021年35期)2021-04-19 12:24:18
考試與評價·高一版(2020年6期)2020-11-02 02:45:24
媽媽寶寶(2019年10期)2019-10-26 02:45:34
中國生殖健康(2019年3期)2019-02-01 06:12:26
鐵道通信信號(2018年11期)2019-01-19 01:15:08
電子制作(2018年11期)2018-08-04 03:25:42
鐵道通信信號(2018年2期)2018-04-18 12:18:10
鐵道通信信號(2016年11期)2016-06-01 12:11:32
鑿巖機械氣動工具(2016年3期)2016-03-01 04:00:25
中國病理生理雜志(2015年8期)2015-12-21 12:38:06
