睪丸微石癥對于成年男性精液質量的影響
2018-03-22 08:57:35毛衛(wèi)林
中國男科學雜志 2018年1期
關鍵詞:研究
毛衛(wèi)林
湖北民族學院附屬民大醫(yī)院泌尿外科(湖北恩施 445000)
睪丸微石癥(Testicular microlithiasis,TM),一種較為罕見的男性生殖系統(tǒng)疾病,主要病理特征為生精小管鈣沉積[1]。目前,TM的主要診斷方法是陰囊超聲檢查[2],而單純的體格檢查準確率較差,容易造成誤診[3]。TM的超聲影像學特征主要是可見彌散于陰囊中直徑約為1~2mm的明亮點狀回聲灶,即鈣化的病灶。睪丸微結石可以隨機分布于整個睪丸中或僅存在于睪丸實質的某塊區(qū)域,根據這個特點可以將TM分為兩種不同的類型:(1)經典型睪丸微石癥(classic testicular microlithiasis, CTM),(2)局限性睪丸微石癥(limited testicular microlithiasis, LTM)[4]。近年來還沒有文獻對國內的TM患病率作過準確統(tǒng)計分析,Decastro等于2008年對1504個志愿者做了前瞻性研究,結果表明通過陰囊超聲掃描檢測發(fā)現TM的患病率為5.6%[5]。而且,有研究表明TM與精子的產生和功能障礙有密切相關[6],因此亟需探究TM的臨床特征及其與精子產生障礙、精子質量的關系,尤其是不同類型TM(CTM, LTM)對精子質量的影響。
資料與方法
一、一般資料
選取2014年至2015年期間到本院生殖醫(yī)學中心檢測的男性患者共150例為研究對象,通過對其陰囊進行超聲波檢查確診CTM共90例,LTM共60例;無男性生殖系統(tǒng)疾病僅接受常規(guī)精液檢查的健康志愿者(對照組)共90例(排除既往睪丸外傷或行外科手術、激素水平紊亂、不孕不育、少精癥、長期飲酒等不良嗜好)。研究之前所有研究對象簽署知情同意書,并進行陰囊超聲檢查。3組病例的一般資料如表1所示,3組患者的年齡、身體質量指數(body mass index, BMI)相較差異均無統(tǒng)計學意義(P>0.05);CTM組分別和LTM組、對照組的睪丸體積比較,差異均具統(tǒng)計學意義(P<0.05)。
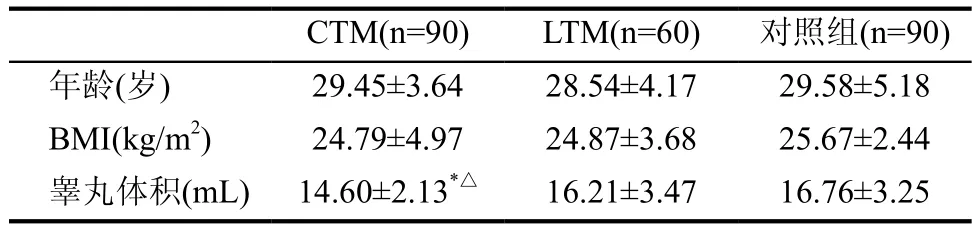
表1 CTM組、LTM組和對照組病例的一般資料
二、陰囊超聲檢查方法
陰囊超聲檢查由一位具有3年以上臨床經驗的超聲檢查師操作,超聲時使用高頻縱、橫剖面探針(中心頻率為7.5MHz,美國GE公司Voluson 730四維彩超儀),并記錄各組人員的睪丸體積(長度、寬度、高度),睪丸體積計算公式為長度×寬度×高度×0.71。實時觀測睪丸各處的回聲反射,主要包括回聲圖形的異質性、結節(jié)、回聲光點等。(1)CTM的診斷標準:一側或雙側睪丸發(fā)現至少5個微結石(5個點狀強回聲);(2)LTM的診斷標準:一側或雙測睪丸發(fā)現1~5個微結石(1~5個點狀強回聲)。
三、精液的收集及檢測
收集精液前7d各組人員避免性生活,手淫法收集精液。之后進行精液檢測(依據世界衛(wèi)生組織2010年頒布的第五版人類精液檢查、處理手冊),檢測指標包括精液體積、精子總數、濃度、總活力[包括前向運動精子progressively motile, PR、非前向運動精子non-progressively motile, NP;總活力為(PR+NP)%]、不活動精子(IM)和平均路徑速度、曲線速度、直線速度。
四、數據分析
結 果
一、精液檢測結果
CTM、LTM及對照組的精液指標如表2所示。CTM組與對照組相比,除精子體積、平均路徑速度、曲線速度、直線速度差異無統(tǒng)計學意義以外,其他指標的差異均具有統(tǒng)計學意義(P<0.05);LTM組和對照組相比僅精子濃度和NP%差異有統(tǒng)計學意義,其余指標P均>0.05;CTM組與LTM組相比,除精子體積、平均路徑速度、曲線速度、直線速度以外,其他指標的差異均具有統(tǒng)計學意義(P<0.05)。
表2 CTM、LTM和對照組精液各項指標比較(±s)
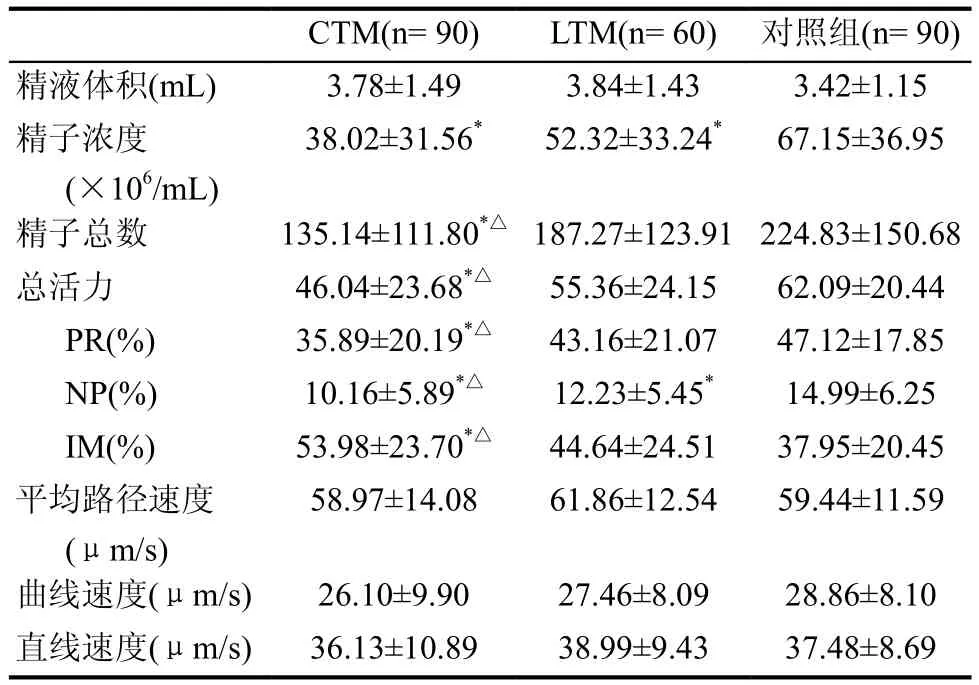
表2 CTM、LTM和對照組精液各項指標比較(±s)
與對照組比較,*為P<0.05;與LTM組比較,△為P<0.05
CTM(n= 90) LTM(n= 60) 對照組(n= 90)精液體積(mL) 3.78±1.49 3.84±1.43 3.42±1.15精子濃度(×106/mL)38.02±31.56* 52.32±33.24* 67.15±36.95精子總數 135.14±111.80*△ 187.27±123.91 224.83±150.68總活力 46.04±23.68*△ 55.36±24.15 62.09±20.44 PR(%) 35.89±20.19*△ 43.16±21.07 47.12±17.85 NP(%) 10.16±5.89*△ 12.23±5.45* 14.99±6.25 IM(%) 53.98±23.70*△ 44.64±24.51 37.95±20.45平均路徑速度(μm/s)58.97±14.08 61.86±12.54 59.44±11.59曲線速度(μm/s) 26.10±9.90 27.46±8.09 28.86±8.10直線速度(μm/s) 36.13±10.89 38.99±9.43 37.48±8.69
討 論
睪丸微石癥(TM)是一種較為罕見的男性生殖系統(tǒng)疾病,在1970年由Priebe等首次發(fā)現并報道[7]。之后Doherty等[8]對超聲技術進行了報道,H?barth等在一次大規(guī)模研究中通過對1710例志愿者進行睪丸超聲檢查后發(fā)現TM的發(fā)生率為0.6%[9]。本研究選取150例研究對象行睪丸超聲檢測,其中有90例(占60%)被確診為CTM,60例為LTM。TM通常在睪丸常規(guī)超聲檢測中被偶然發(fā)現,已有文獻報道其與不孕不育存在密切聯(lián)系[10-12]。TM作為一種睪丸生殖障礙綜合征,可影響男性的生育能力,包括不育、睪丸萎縮及其他生殖異常等[13]。患有TM的男性患者一般會出現精子數量劇減[14],精子活力下降,從而導致生育能力下降。TM不但會導致生精小管阻塞,而且會影響睪丸的血液輸送。有研究表明發(fā)生TM的原因可能是生精小管內細胞的變性退化[15],患有TM的男性在接受睪丸超聲檢查時會出現異常回聲,便可判斷結石位置和數量,微結石會隨機分散于睪丸實質造成生精小管堵塞[12]。
本研究發(fā)現CTM和LTM患者的精子各項指標低于對照組,本研究結果印證了TM造成精子功能低下,包括減少產精量、減少精子濃度、降低精子活力、移動速率等。這與以往的研究結果一致。Thomas等[16]證實TM與精子功能低下密切相關,Lenz等[17]的研究也曾報道TM會顯著影響精子產生,造成精子總量減少甚至睪丸萎縮,綜合以上研究結果:微結石彌散地分布于CTM患者的雙側睪丸實質中,而LTM患者僅睪丸實質的某側或某處能發(fā)現微結石,說明TM的程度與男性的精液質量呈正相關。正好解釋了CTM患者的精液質量顯著低于LTM患者的原因。
本研究中發(fā)現CTM的發(fā)病率高于LTM,根據現有報道仍無法對CTM和LTM的患病率高低下定論[18,19],有待于未來更多的研究來確定不同類型TM的發(fā)病率。目前在臨床上仍未發(fā)現有效治療TM的方法[12],Korde等[20]認為TM可作為睪丸疾病的標志物,應對患者進行后續(xù)隨訪,但是由于目前仍未見報道TM導致睪丸惡性腫瘤,所以在臨床上鮮有主動的后續(xù)隨訪。本研究證實TM與成年男性的精液質量密切相關,TM的程度能正相關地降低男性精液的質量,降低精子活力和移動能力,同時發(fā)現CTM患者的精液質量顯著差于LTM患者。
在未來的研究中,我們會對TM確診患者進行后續(xù)追蹤,觀察其睪丸的組織學變化,研究TM不同階段對精液質量的影響。
1 Poyrazoglu S, Saka N, Agayev A, et al. Prevalence of testicular microlithiasis in males with congenital adrenal hyperplasia and its association with testicular adrenal rest tumors. Horm Res P?diatr 2010; 73(6): 443-448
2 Sakamoto H, Shichizyou T, Saito K, et al. Testicular microlithiasis identified ultrasonographically in Japanese adult patients: prevalence and associated conditions.Urology 2006; 68(3): 636-641
3 Serter S, Gümü? B, Unlü M,, et al. Prevalence of testicular microlithiasis in an asymptomatic population. Scand J Urol Nephrol 2006; 40(3): 212-214
4 Yee WS, Kim YS, Kim SJ, et al. Testicular microlithiasis:prevalence and clinical signi fi cance in a population referred for scrotal ultrasonography. Korean J Urol 2011; 52(3):172-177
5 De castro BJ, Peterson AC, Costabile RA. A 5-Year Followup Study of Asymptomatic Men With Testicular Microlithiasis. J Urol 2008; 179(4): 1420-1423
6 La Vignera S, Condorelli R, Vicari E, et al. Testicular microlithiasis: analysis of prevalence and associated testicular cancer in central-eastern Sicilian andrological patients. Andrologia 2012; 44 Suppl 1: 295-299
7 Priebe CJ Jr, Garret R. Testicular calci fi cation in a 4-year-old boy. Pediatrics 1970; 46(5): 785-788
8 Doherty JR, Trahey GE, Nightingale KR, et al. Acoustic radiation force elasticity imaging in diagnostic ultrasound.IEEE Trans Ultrason Ferroelectr Freq Control 2013; 60(4):685-701
9 H?barth K, Susani M, Szabo N, et al. Incidence of testicular microlithiasis. Urology 1992; 40(5): 464-467
10 Sakamoto H, Saito K, Shichizyo T, et al. Color Doppler ultrasonography as a routine clinical examination in male infertility. In J Urol 2006; 13(8): 1073-1078
11 Qublan HS, Al-Okoor K, Al-Ghoweri AS, et al.Sonographic spectrum of scrotal abnormalities in infertile men. J Clin Ultrasound 2007; 35(8): 437-441
12 Zhang QH, Lu GS, Shen XC, et al. Nanobacteria May Be Linked to Testicular Microlithiasis in Infertility. J Androl 2009; 31(2): 121-125
13 Tan MH, Eng C. Testicular microlithiasis: recent advances in understanding and management. Nat Rev Urol 2011;8(3): 153-163
14 Dutra RA, Perez-Bóscollo AC, Melo EC, et al. Clinical importance and prevalence of testicular microlithiasis in pediatric patients. Acta Cir Bras 2011; 26(5): 387-390
15 Chiang LW, Yap TL, Asiri MM, et al. Implications of incidental finding of testicular microlithiasis in paediatric patients. J Pediatr Urol 2012; 8(2): 162-165
16 Thomas K, Wood SJ, Thompson AJ, et al. The incidence and significance of testicular microlithiasis in a subfertile population. Br J Radiol 2000; 73(869): 494-497
17 Lenz S, Thomsen JK, Giwercman A, et al. Ultrasonic texture and volume of testicles in infertile men. Hum Reprod 1994; 9(5): 878-881
18 Middleton WD, TeefeySA, Santillan CS. Testicular microlithiasis: prospective analysis of prevalence and associated tumor. Radiology 2002; 224(2): 425-428
19 Bennett HF, Middleton WD, Bullock AD, et al. Testicular microlithiasis: US follow-up. Radiology 2001; 218(2): 359-363
20 Korde LA, Premkumar A, Mueller C, et al. Increased prevalence of testicular microlithiasis in men with familial testicular cancer and their relatives. Br J Cancer 2008;99(10): 1748-1753
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
天津外國語大學學報(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
科技傳播(2019年22期)2020-01-14 03:06:54
遼金歷史與考古(2019年0期)2020-01-06 07:45:20
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
電子制作(2018年11期)2018-08-04 03:26:04
汽車工程學報(2017年2期)2017-07-05 08:13:02
國際商務財會(2017年8期)2017-06-21 06:14:14
電子制作(2017年23期)2017-02-02 07:17:19