硬膜外鎮痛分娩中發生持續性枕后位的臨床分析
2020-06-11 00:42:07李利平
中外醫療 2020年5期

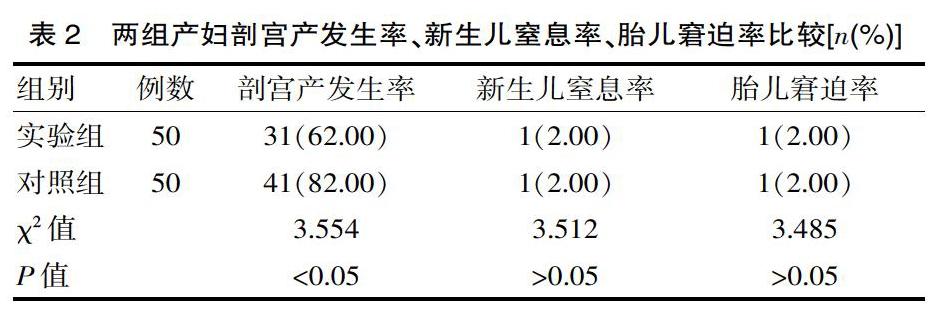
[摘要] 目的 觀察分析硬膜外鎮痛分娩中發生持續性枕后位臨床情況(枕后位發生率、母嬰解決以及臨床分娩方式)。方法 方便選取該院在2017年1月—2019年2月收治的100例產婦,按照有無接受硬膜外鎮痛分娩分為實驗組(50例,接受硬膜外鎮痛分娩)和對照組(50例,未接受硬膜外鎮痛分娩)。采用統計學分析兩組產婦的持續性枕后位發生率、母嬰結局。 結果 實驗組產婦的持續性枕后位發生率、第一產程催產素使用率、第二產程催產素使用率、產后平均出血量分別為12.00%、60.00%、32.00%、(200.02±100.15)mL,對照組分別為10.00%、30.00%、30.00%、(290.36±110.38)mL,兩組產婦的持續性枕后位發生率、第二產程催產素比較差異無統計學意義(χ2=10.455、10.212,P>0.05),實驗組產婦第一產程催產素使用率高于對照組(χ2=5.993,P<0.05),實驗組產婦產后平均出血量顯著少于對照組(t=18.326,P<0.05);實驗組新生兒窒息率、胎兒窘迫率、新生兒出生體重分別為2.00%、2.00%、(3.26±0.21)kg,對照組分別為2.00%、2.00%、(3.30±0.14)kg,兩組新生兒窒息率、胎兒窘迫率、新生兒出生體重比較差異無統計學意義(χ2=3.512、3.485、3.522,P>0.05);實驗組產婦剖宮產發生率為62.00%,對照組為82.00%,實驗組產婦剖宮產發生率顯著低于對照組(χ2=3.554,P<0.05)。結論 硬膜外鎮痛分娩可有效改善母嬰結局。
[關鍵詞] 硬膜外鎮痛;分娩;持續性枕后位;母嬰結局
[中圖分類號] R5? ? ? ? ? [文獻標識碼] A? ? ? ? ? [文章編號] 1674-0742(2020)02(b)-0048-03
Clinical Analysis of Persistent Occipital Posterior Position in Epidural Analgesia during Delivery
LI Li-ping
Department of Anesthesiology, Changsha Maternal and Child Health Hospital, Changsha, Hunan Province, 410007 China
[Abstract] Objective To observe and analyze the clinical situation of persistent occipital posterior position in epidural analgesia delivery (incidence of occipital posterior position, maternal and infant solutions and clinical delivery mode). Methods A total of 100 parturients admitted to our hospital (from January 2017 to February 2019) were convenienty selected and divided into an experimental group (50 parturients who received epidural analgesia) and a control group (50 parturients who did not receive epidural analgesia). Statistics were used to analyze the incidence of persistent posterior occipital position and maternal and infant outcomes in the two groups. Results Experimental group the incidence of persistent pillow after a maternal, the first stages of oxytocin utilization, the second labor oxytocin average utilization rate, postpartum blood loss were 12.00%, 60.00%, 32.00%, (200.02±100.15)mL, the control group were 10.00%, 30.00%, 30.00%, (290.36±110.38)mL, two groups of maternal persistent pillow after the incidence, the second labor oxytocin is no statistical significance (x2=10.455, 10.212, P>0.05). The utilization rate of oxytocin in the first stage of labor in the experimental group was higher than that in the control group(χ2=5.993, P<0.05), and the average postpartum blood loss in the experimental group was significantly lower than that in the control group(t=18.326, P<0.05). The rates of neonatal asphyxia, fetal distress and neonatal birth weight in the experimental group were 2.00%, 2.00% and (3.26±0.21) kg, respectively, while those in the control group were 2.00%, 2.00% and (3.30±0.14) kg, respectively. There were no statistically significant differences in the rates of neonatal asphyxia, fetal distress and neonatal birth weight in the two groups(χ2=3.512, 3.485,3.522, P>0.05). The incidence of cesarean section was 62.00% in the experimental group and 82.00% in the control group. The incidence of cesarean section in the experimental group was significantly lower than that in the control group(χ2=3.554, P<0.05). Conclusion Epidural analgesia can improve maternal and infant outcomes.
該文研究結果顯示,實驗組產婦產后平均出血量顯著少于對照組(P<0.05)。子宮收縮可有益于胎頭內旋轉,如果子宮收縮力道不足,會難以旋轉胎頭。雖然硬膜外鎮痛分娩方式所面臨的持續性枕后位概率較高,但是只要在硬膜外鎮痛過程中注意合理給藥,密切監測宮縮進展情況以及產程發展,及時處理枕后位能夠幫助胎頭旋轉,最終顯著提高自然分娩率,減少術后出血量。該文研究結果顯示實驗組新生兒窒息率、胎兒窘迫率、新生兒出生體重分別為2.00%、2.00%、(3.26±0.21)kg,對照組分別為2.00%、2.00%、(3.30±0.14)kg,兩組新生兒窒息率、胎兒窘迫率、新生兒出生體重比較差異無統計學意義(P>0.05)。翟利平[8]在相關研究中顯示,治療結束后新生兒窒息率為1.00%,胎兒窘迫率為2.00%,新生兒出生體重為(3.33±0.15)kg,與該文研究結果保持高度一致。在產婦分娩過程中,不管有無接受硬膜外鎮痛分娩方式,助產士或者醫師均需要幫助產婦及時糾正宮縮乏力情況,積極指導產婦正確用力,可顯著降低新生兒窒息率、胎兒窘迫率。
綜上所述,硬膜外鎮痛分娩可顯著提高第一產程催產素使用率、第二產程催產素使用率,減少產后平均出血量,提高母嬰生活質量。
[參考文獻]
[1]? 楊同文,熊巍,任自剛,等.系統評價硬膜外分娩鎮痛時機對初產婦分娩過程的影響:Meta分析[J].臨床和實驗醫學雜志,2018,17(11):1206-1212.
[2]? Vincenzo Zanardo,Francesca Volpe,Matteo Parotto,et al.Nitrous oxide labor analgesia and pain relief memory in breast feeding women[J].The Journal of Maternal-Fetal & Neonatal Medicine,2018,31(24):3243-3248.
[3]? 李瑞,羅志鍇,楊麗珍,等.不同濃度羅哌卡因復合舒芬太尼在硬膜外鎮痛分娩中的效果評價[J].實用臨床醫藥雜志,2018,22(23):82-84,87.
[4]? 王芳,姜文,邢梅,等.腰硬聯合麻醉復合術后硬膜外鎮痛對足月妊娠初產婦無痛分娩產程時間及術后血清PRL、tPA水平的影響[J].中國醫學前沿雜志:電子版,2018,10(8):60-64.
[5]? 楊會義,安麗,許萍,等.右美托咪定用于妊娠期高血壓產婦硬膜外分娩鎮痛的療效及護理方式[J].河北醫藥,2017,39(11):1746-1748.
[6]? 李冰,陳緒軍,郭艷,等.不同濃度羅哌卡因復合舒芬太尼在硬膜外階梯式分娩鎮痛中的應用[J].臨床麻醉學雜志,2016, 32(4):361-365.
[7]? 宗銀東,聶穎,姜義鐵,等.羅哌卡因硬膜外患者自控鎮痛的無痛分娩效果及應激反應的臨床研究[J].重慶醫學,2016, 45(17):2407-2409.
[8]? 翟利平,徐公元,鄧愛華,等.不同時機實施硬膜外鎮痛分娩對母嬰結局的影響[J].中國婦幼保健,2017,32(15):3688-3690.
(收稿日期:2019-11-10)
[作者簡介] 李利平(1986-),女,湖南長沙人,碩士,主治醫師,研究方向:鎮痛分娩,單肺通氣。
