綿陽地區ICU危重患者康復活動情況調查分析
2020-10-29 05:38:50何海燕康秀華
醫學信息
2020年18期
何海燕 康秀華

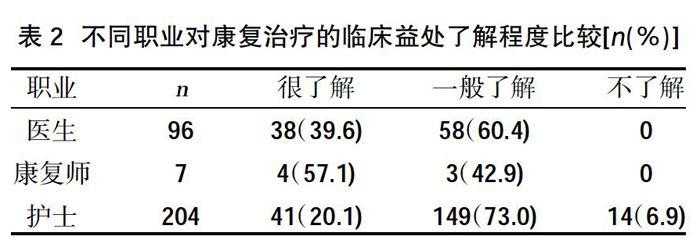
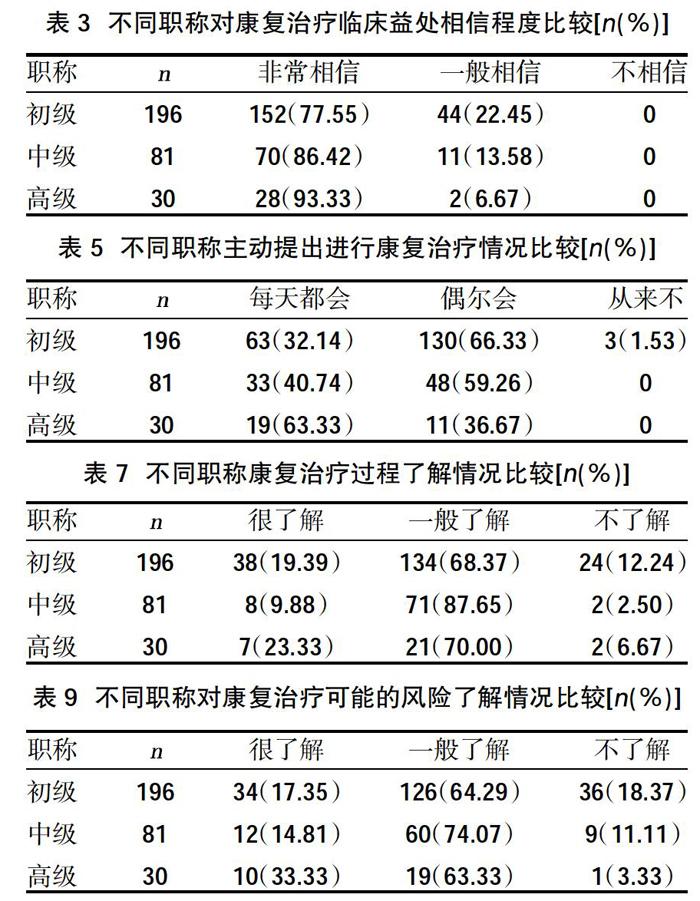
摘要:目的 ?調查綿陽地區所有醫院ICU危重患者康復活動情況,探索適合本地區ICU環境的標準化早期康復方案。方法 ?于2019年11月18~20日,采用整群抽樣法對轄區ICU醫務人員進行線上問卷星調查,采用自制問卷,分析一般資料、醫院配置情況、ICU危重患者康復治療情況及不同職稱與職業醫護人員對重癥康復情況。結果 ?共22家ICU 307名醫護人員參與了此次調查,醫生96名,護士204名,康復治療師7名,職稱以初級職稱為主,醫院等級以二甲為主。未每天配備康復治療師的ICU占比81.82%,醫生床位比平均0.42∶1,護士床位比平均1.69∶1,區域內ICU有可用的康復輔助工具的占比45.45%。僅22.73%的ICU常規每天開展危重患者康復活動,康復治療主要由醫師臨床決策,康復師和護士主要參與,僅13.64%的ICU有康復治療流程圖及知情同意書。職稱與康復治療的臨床益處了解程度呈正相關(P<0.05);不同職業對康復治療的臨床益處了解程度比較,差異有統計學意義(P<0.05)。職稱與對康復治療臨床益處相信程度呈升高趨勢(P<0.05),不同職業醫護人員對康復治療臨床益處相信程度比較,差異無統計學意義(P>0.05)。職稱與主動提出進行康復治療頻數呈正相關(P<0.05);不同職業醫護人員主動提出康復治療的頻率比較,差異有統計學意義(P<0.05)。職稱與醫護人員對康復治療過程的了解程度無相關性(P>0.05);不同職業醫護人員對康復過程的了解程度間比較,差異有統計學意義(P<0.05)。職稱等級與了解程度間呈正相關(P<0.05);不同職業對康復治療可能的風險了解程度比較,差異有統計學意義(P<0.05)。結論 ?ICU危重患者康復活動開展需加強配置,提高醫務人員對危重癥患者康復活動的認識,制定適合本地區ICU環境的標準化早期康復方案。
關鍵詞:ICU;危重患者;康復活動
中圖分類號:R19 ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? 文獻標識碼:A ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? DOI:10.3969/j.issn.1006-1959.2020.18.038
文章編號:1006-1959(2020)18-0118-04
Investigation and Analysis of Rehabilitation Activities of Critically Ill Patients
in ICU in Mianyang Area
HE Hai-yan,KANG Xiu-hua
(Department of Critical Care Medicine,Mianyang Central Hospital,Mianyang 621000,Sichuan,China)
Abstract:Objective ?To investigate the rehabilitation activities of critically ill patients in ICUs in all hospitals in Mianyang area, and to explore standardized early rehabilitation programs suitable for the ICU environment in the region.Methods ?From November 18 to 20, 2019, a cluster sampling method was used to conduct an online questionnaire survey of ICU medical staff in the jurisdiction. A self-made questionnaire was used to analyze general information, hospital configuration, ICU rehabilitation and treatment of critically ill patients, and different professional titles. Occupational medical staff recover from severe illness.Results ?A total of 307 medical staff from 22 ICUs participated in the survey. There were 96 doctors, 204 nurses, and 7 rehabilitation therapists. Their professional titles were junior titles, and the hospital's grades were mainly Grade A. The proportion of ICUs not equipped with rehabilitation therapists every day accounted for 81.82%, the average doctor bed ratio was 0.42:1, the average nurse bed ratio was 1.69:1, and 45.45% of the ICUs in the region had available rehabilitation aids. Only 22.73% of ICUs routinely carry out rehabilitation activities for critically ill patients every day. Rehabilitation treatment was mainly determined by the clinical decision-making of physicians, with the main participation of rehabilitation practitioners and nurses. Only 13.64% of ICUs had rehabilitation treatment flowcharts and informed consent. The professional title was positively correlated with the degree of understanding of the clinical benefits of rehabilitation treatment (P<0.05); the difference in the degree of understanding of the clinical benefits of rehabilitation treatment in different occupations was statistically significant (P<0.05). The professional title and the degree of belief in the clinical benefits of rehabilitation treatment showed an increasing trend (P<0.05). There was no statistically significant difference in the degree of belief among medical staff of different occupations in the clinical benefits of rehabilitation (P>0.05). The professional title was positively correlated with the frequency of active rehabilitation (P<0.05); the frequency of active medical staff in different occupations compared with the frequency of active rehabilitation, the difference was statistically significant (P<0.05). There was no correlation between the professional title and the medical staff's understanding of the rehabilitation process (P>0.05); the difference between the medical staff's understanding of the rehabilitation process of different occupations was statistically significant (P<0.05). There was a positive correlation between the level of professional title and the degree of understanding (P<0.05); the difference in the degree of understanding of possible risks of rehabilitation therapy in different occupations was statistically significant (P<0.05).Conclusion ?It was necessary to strengthen the deployment of rehabilitation activities for critically ill patients in ICU, improved medical staff's awareness of rehabilitation activities for critically ill patients, and formulated standardized early rehabilitation programs suitable for the ICU environment in the region.
Key words:ICU;Citically ill patients;Rehabilitation activities
ICU重癥患者早期活動和康復訓練可促進機體功能恢復,減少譫妄的發生、縮短機械通氣時間和ICU住院時間,其安全性、有效性、可行性已得到充分證明[1]。我國ICU重癥患者早期活動和康復訓練尚處于初期發展和摸索階段,實踐現狀并不理想,尚無統一的康復標準和康復流程[2]。為更好地推廣和實施ICU早期康復治療,改善ICU患者臨床結局,降低醫療費用,本研究調查了綿陽地區危重患者康復活動情況,旨在探索適合本地區ICU環境的標準化早期康復方案,現報道如下。……
登錄APP查看全文