三種干擾素γ釋放試驗在不同年齡結核病患者中的應用比較
2020-10-29 05:38:50美朗曲措陳民黃麗萍邊瑪措
醫學信息
2020年18期
關鍵詞:方法
美朗曲措 陳民 黃麗萍 邊瑪措
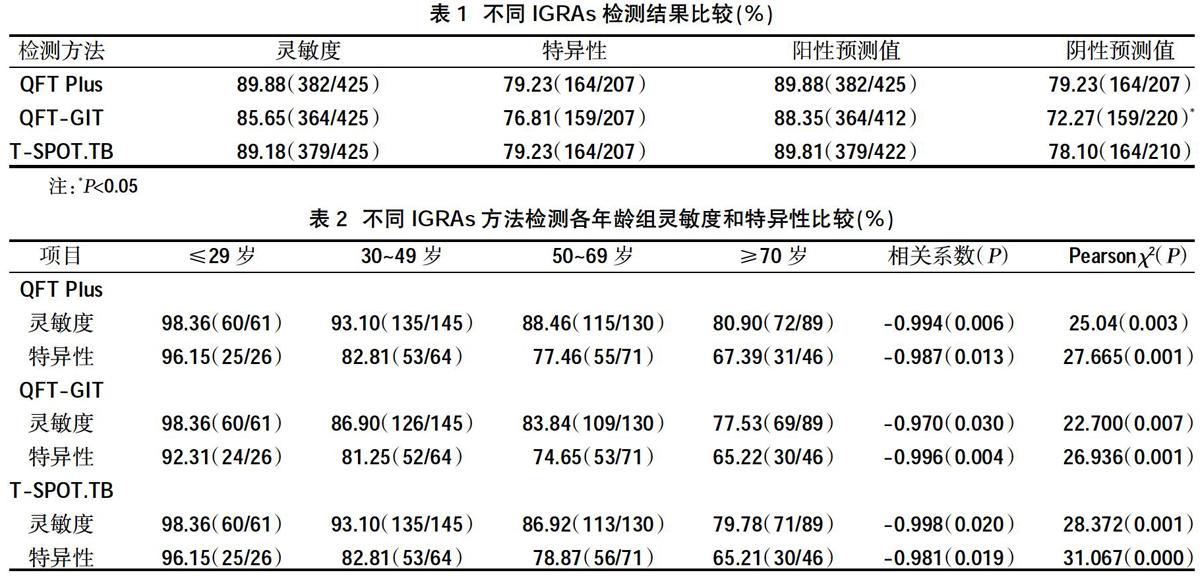
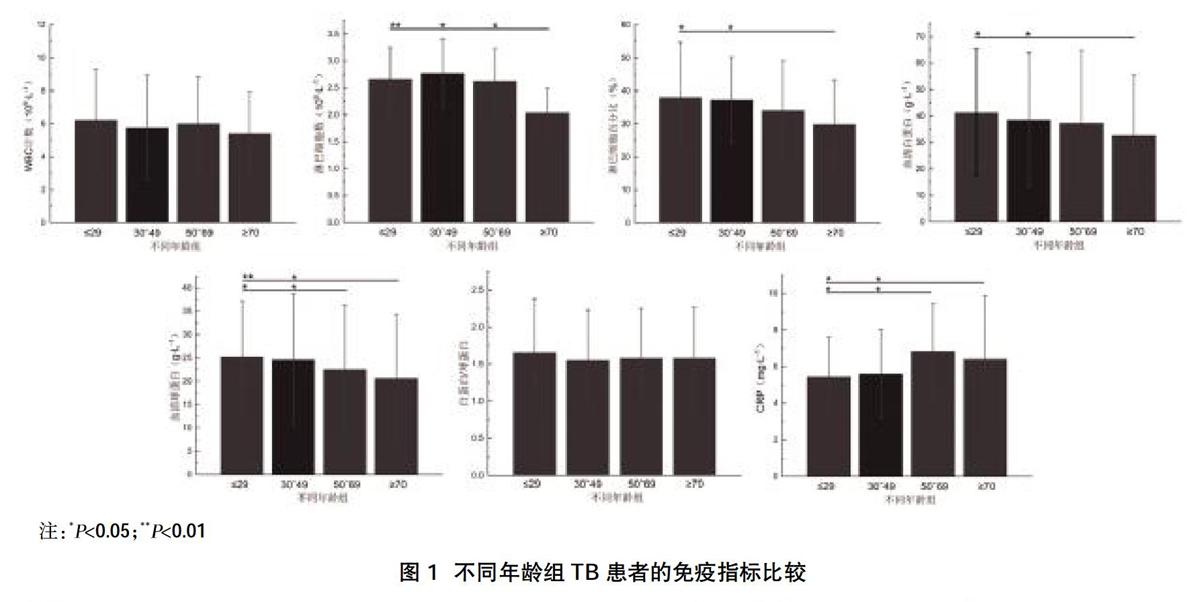

摘要:目的 ?比較三種干擾素γ釋放試驗在不同年齡結核病(TB)患者中的應用效果。方法 ?選取2016年6月~2019年11月西藏自治區人民醫院確診為TB患者425例,按照年齡分為≤29歲61例,30~49歲145例,50~69歲130例,≥70歲89例,均進行三種IGRAs(QFT Plus、QFT-GIT及T-SPOT.TB)檢測,比較三種方法檢測結果及其在各年齡組靈敏度和特異性,并分析IGRAs檢測不同年齡段TB患者免疫指標結果。結果 ?不同IGRAs方法的靈敏度、特異性、陽性預測值比較,差異無統計學意義(P>0.05),而QFT-GIT方法的陰性預測值低于QFT Plus和T-SPOT.TB方法,差異有統計學意義(P<0.05)。不同IGRAs方法檢測各年齡段的靈敏度和特異性比較,差異有統計學意義(P<0.05);根據雙變量回歸分析,靈敏度、特異性與年齡均呈負相關(P<0.05)。不同年齡組TB患者WBC數和白蛋白/球蛋白比值比較,差異無統計學意義(P>0.05)。≥70歲年齡組TB患者淋巴細胞數、淋巴細胞百分比、血清白蛋白數較其他年齡組TB患者下降(P<0.05),CRP較其他年齡組TB患者上升(P<0.05)。結論對于<70歲TB患者,QFT Plus及T-SPOT.TB可用于TB早期診斷工具,而≥70歲TB患者,仍需結合痰涂片、痰結核菌DNA、影像學檢查等手段綜合判斷。
關鍵詞:IGRAs;QFT Plus;QFT-GIT;T-SPOT.TB;結核診斷
中圖分類號:R52 ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ?文獻標識碼:A ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ?DOI:10.3969/j.issn.1006-1959.2020.18.055
文章編號:1006-1959(2020)18-0164-04
Application Comparison of Three Kinds of Interferon γ Release Test
in Tuberculosis Patients of Different Ages
MEILANG Qu-cuo,CHEN Min,HUANG Li-ping,BIAN Ma-cuo
(Department of Respiratory Medicine,People's Hospital of Tibet Autonomous Region,Lhasa 850000,Tibet,China)
Abstract:Objective ?To compare the effects of three interferon gamma release tests in tuberculosis (TB) patients of different ages.Methods ?From June 2016 to November 2019, 425 patients with TB diagnosed in the People's Hospital of Tibet Autonomous Region were selected. According to age, 61 cases were ≤29 years old, 145 cases were 30-49 years old, 130 cases were 50-69 years old, and 89 were ≥70 years old. In each case,3 types of IGRAs (QFT Plus, QFT-GIT and T-SPOT.TB) were tested,compare the detection results of the three methods and their sensitivity and specificity in each age group, and analyze the results of IGRAs detecting immune indicators in TB patients of different ages.Results ?The sensitivity, specificity, and positive predictive value of different IGRAs methods were not statistically different (P>0.05), while the negative predictive value of QFT-GIT method was lower than that of QFT Plus and T-SPOT.TB methods,the difference was statistically significant(P<0.05). The sensitivity and specificity of different IGRAs methods for detecting each age group were compared,the difference was statistically significant(P<0.05); according to the bivariate regression analysis, the sensitivity and specificity were negatively correlated with age (P<0.05). There was no statistically significant difference in WBC count and albumin/globulin ratio in TB patients of different age groups (P>0.05). The number of lymphocytes, the percentage of lymphocytes, and the number of serum albumin in TB patients in the age group ≥70 years were lower than those in TB patients in other age groups (P<0.05), and CRP was higher than that in TB patients in other age groups (P<0.05).Conclusion ?For TB patients under 70 years of age, QFT Plus and T-SPOT.TB can be used as early diagnostic tools for TB, while TB patients ≥ 70 years of age still need to be combined with sputum smears, sputum tuberculosis DNA, imaging examination and other methods to make comprehensive judgments.
Key words:IGRAs;QFT Plus;QFT-GIT;T-SPOT.TB;Tuberculosis diagnosis
結核病(tuberculosis,TB)是一種威脅人類健康的傳染性疾病,世界范圍內每年新增約610萬結核病例,其中約有180萬例死亡[1],因此結核病的早期準確診斷對控制其傳播至關重要。干擾素γ釋放試驗(IGRA)是一種能夠克服傳統結核菌素皮膚試驗(TST)局限性的診斷方法[2-4]。目前常見商品化IGRA試劑盒有QuantiFERONTB Gold Plus(QFT Plus)、QuantiFERON-TB-GoldIn-Tube(QFT-GIT)和T-SPOT.TB試劑盒。QFT Plus是新一代QFT-GIT,于2015年推出[5],QFT-GIT含有一個TB特異性抗原管,通過酶聯免疫吸附試驗測定γ干擾素(IFN-γ)的濃度[6],而QFT Plus試劑盒由兩個TB特異性抗原管組成[7,8];T-SPOT.TB則是通過酶聯免疫斑點試驗測量IFN-γ分泌的T細胞數量[9]。這三種IGRA均與IFN-γ緊密相關,而IFN-γ的產生與人體免疫相關,隨著年齡的增長,人體的免疫反應強度下降[10,11]。本研究旨在比較三種干擾素γ釋放試驗在不同年齡結核病(TB)患者中的應用效果,現報道如下。
1資料與方法
1.1一般資料 ?選取2016年6月~2019年11月西藏自治區人民醫院確診(門診及住院)的肺結核(TB)患者425例,該研究經我院醫學倫理委員會批準,參與研究者均簽署知情同意書。所有……
登錄APP查看全文
猜你喜歡
中老年保健(2021年9期)2021-08-24 03:52:04
河北畫報(2021年2期)2021-05-25 02:07:46
中學生數理化(高中版.高考理化)(2020年2期)2020-04-21 05:33:04
兒童繪本(2020年5期)2020-04-07 17:46:30
兒童故事畫報(2019年5期)2019-05-26 14:26:14
Coco薇(2016年2期)2016-03-22 02:42:52
山東青年(2016年1期)2016-02-28 14:25:23
Coco薇(2015年1期)2015-08-13 02:47:34
小雪花·成長指南(2015年7期)2015-08-11 15:03:12
小雪花·成長指南(2015年4期)2015-05-19 14:47:56