腦性癱瘓患者術后躁動的相關因素①
2014-05-08 06:35:38劉海泉王增春王強任自剛熊巍
中國康復理論與實踐 2014年5期
關鍵詞:手術
劉海泉,王增春,王強,任自剛,熊巍
腦性癱瘓患者術后躁動的相關因素①
劉海泉,王增春,王強,任自剛,熊巍
目的探討腦癱患者術后躁動的原因。方法回顧分析199例在靜吸復合全麻下接受選擇性后根切斷術或下肢矯形術腦癱患者的臨床資料。結果術后30例患者發生躁動(15%),躁動組患者的年齡較小(P<0.05)、體重較輕(P<0.01)、單位時間及單位體重下所使用的鎮痛藥物較少(P<0.01)。結論術中及術后充分鎮痛以及術前必要的心理干預及鎮靜藥物可能會減少術后躁動的發生率。
腦性癱瘓;術后躁動;疼痛
[本文著錄格式] 劉海泉,王增春,王強,等.腦性癱瘓患者術后躁動的相關因素[J].中國康復理論與實踐,2014,20(5): 414-416.
手術是解除腦癱患者下肢痙攣的一種有效方法,這類手術通常在靜吸復合全麻下進行。術后躁動是圍麻醉期的一種嚴重并發癥,它不僅增加患者受到意外傷害的危險性,而且會延長麻醉恢復期的監護時間,增加醫療費用。本研究回顧接受手術的腦癱患者的臨床資料,探討可能導致術后躁動的相關因素。
1 資料與方法
1.1 一般資料
2008年1月~2013年9月收入北京博愛醫院骨關節康復科或脊柱脊髓外科,并在靜吸復合全麻下接受腰段選擇性脊神經后根切斷術(selective posterior rhizotomy,SPR)或下肢矯形術(lower limbs orthopedics,LLO)的腦癱患者199例,其中男性141例,女性58例;年齡2~37歲,平均(11.24±6.112)歲;體重12~93 kg,平均(32.19±15.091)kg;痙攣型186例,混合型13例。
所有患者術前常規禁食8 h,禁飲6 h;入室后常規監測血壓、心電圖、脈搏血氧飽和度(pulse blood oxygen saturation,SpO2),建立靜脈通道。患者若嚴重哭鬧不配合,予氯胺酮肌肉注射或異氟醚或七氟醚面罩吸入。麻醉誘導予咪唑安定0.04 mg/kg、丙泊酚2 mg/kg、維庫溴銨 0.1 mg/kg或羅庫溴銨 0.5~0.6 mg/kg、芬太尼2 μg/kg或舒芬太尼0.4 μg/kg、地塞米松5~10 mg。術中吸入O2-N2O-異氟醚或O2-N2O-七氟醚混合氣體,濃度是1.3肺泡最低有效濃度(minimum alveolar concentration,MAC),間隔40 min靜脈給予芬太尼誘導量1/3~1/4,或持續泵入舒芬太尼0.1~0.2 μg/ kg·h。手術過程中保持腦電雙頻指數(bispectral index,BIS)50~60,以防止術中知曉。手術結束縫皮時停止應用吸入和靜脈麻醉藥。
1.2 觀察指標
查閱病歷及麻醉不良事件記錄,記錄患者一般情況,手術類型,麻醉時間,手術時間,麻醉前是否嚴重哭鬧,術中是否使用七氟醚、阿片類鎮痛藥類型及其劑量,以及不良事件中是否有麻醉蘇醒期躁動。
1.3 統計學分析
2 結果
共有30例出現麻醉蘇醒期躁動(躁動組)。躁動組與非躁動組在性別、腦癱類型、手術方式、麻醉時間、手術時間、術中鎮痛藥物種類、麻醉氣體選擇方面無顯著性差異(P>0.05);在年齡、體重、術中鎮痛藥物劑量、術前有無嚴重哭鬧方面存在顯著性差異,躁動組患者年齡較小(P<0.05)、體重較輕(P<0.01)、單位時間及單位體重下所使用的鎮痛藥物較少(P<0.01)。見表1。
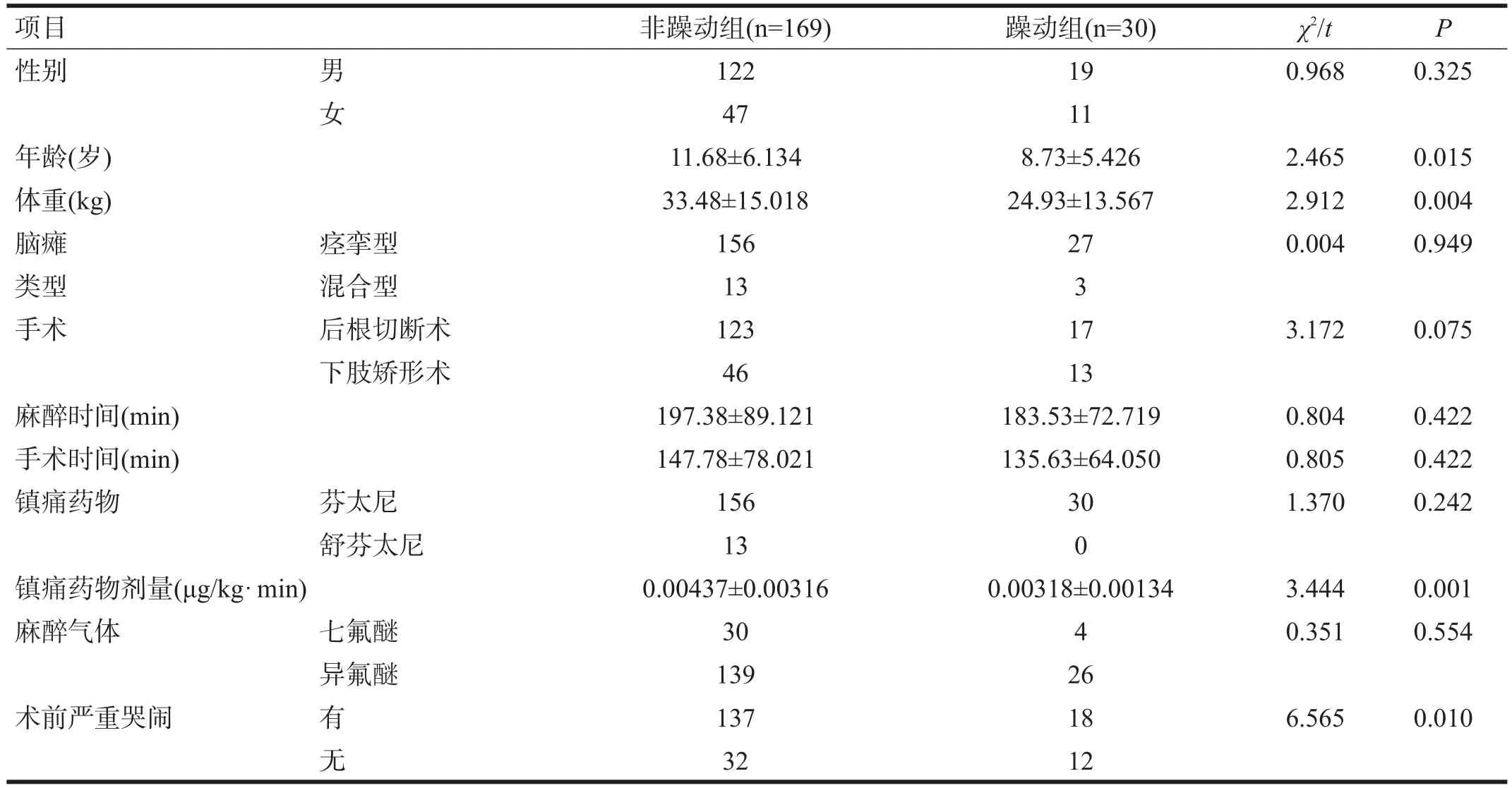
表1 非躁動組與躁動組的臨床資料比較
3 討論
術后躁動的發病率并不一致。成人的發病率可達21%[1];兒童的發病率變化較大,一般為10%~67%[2]。本組資料中,術后躁動發病率15%,與之基本符合。
目前術后躁動的病因還并不清楚,但有一些因素可能與其發生有關,如術后疼痛、麻醉蘇醒過快、患者年齡低、耳鼻喉科手術、術前焦慮以及兒童日常性格[3]。
疼痛被認為是最有可能導致術后躁動的因素,使用鎮痛藥物能夠不同程度降低術后躁動的發生率[4-6]。本研究也發現,躁動組患者所使用的阿片類鎮痛藥物較少,基本上符合這一結論。
年齡是術后躁動的一個危險因素,低齡患者全麻后術后出現躁動的概率較高[7-8]。本研究也發現躁動組患者的年齡低于非躁動組。
術前情緒不穩定與術后躁動有一定的相關性[9-10]。我們發現術前有嚴重哭鬧的患者術后發生躁動的概率較高。術后留置導尿管也可能是麻醉蘇醒后誘發躁動的一個因素,但由于我們觀察的患者均在術后留置導尿管,因此沒有對此因素進行統計分析。
目前很多研究者認為,吸入性麻醉藥七氟醚與術后躁動具有相關性[11-16],雖然機制不清,但大多數認為是由于七氟醚“麻醉蘇醒過快”導致的;但使用“蘇醒更快”的麻醉藥丙泊酚卻并未出現更多的術后躁動事件[17-18],因此麻醉蘇醒過快可能并不是七氟醚麻醉引起術后躁動的原因。本研究并未發現術中使用七氟醚對出現術后躁動產生影響。
動物實驗中發現七氟醚能夠誘導大多數藍斑核神經元產生興奮性內向電流,這可能是七氟醚麻醉具有較高術后躁動發生率的潛在機制[19]。由于腦癱患者在中樞神經系統發育上存在缺陷,這類患者在術后躁動方面是否具有自己的特點有待進一步觀察。
由于術后疼痛、術前情緒不穩定以及低齡患者與術后躁動具有相關性,因此圍麻醉期間使用足夠的鎮痛藥,術前進行有效的心理干預及必要的鎮靜藥可能對降低術后躁動有一定的作用。
[1]Yu D,Chai W,Sun X,et al.Emergence agitation in adults:riskfactors in 2,000 patients[J].Can J Anaesth,2010,57(9): 843-848.
[2]Silva LM,Braz LG,Modolo NS.Emergence agitation in pediatric anesthesia:current features[J].J Pediatr(Rio J),2008,84 (2):107-113.
[3]Vlajkovic GP,Sindjelic RP.Emergence delirium in children: many questions,few answers[J].Anesth Analg,2007,104(1): 84-91.
[4]Li X,Zhang Y,Zhou M,et al.The effect of small dose sufentanil on emergence agitation in preschool children following sevoflurane anesthesia for elective repair of unilateral inguinal hernia[J].Saudi Med J,2013,34(1):40-45.
[5]Dong YX,Meng LX,Wang Y,et al.The effect of remifentanil on the incidence of agitation on emergence from sevoflurane anaesthesia in children undergoing adenotonsillectomy[J].Anaesth Intensive Care,2010,38(4):718-722.
[6]Inomata S,Maeda T,Shimizu T,et al.Effects of fentanyl infusion on tracheal intubation and emergence agitation in preschool children anaesthetized with sevoflurane[J].Br J Anaesth,2010,105(3):361-367.
[7]Saringcarinkul A,Manchupong S,Punjasawadwong Y.Incidence and risk factors of emergence agitation in pediatric patients after general anesthesia[J].J Med Assoc Thai,2008,91 (8):1226-1231.
[8]Nakayama S,Furukawa H,Yanai H.Propofol reduces the incidence of emergence agitation in preschool-aged children as well as in school-aged children:a comparison with sevoflurane[J].JAnesth,2007,21(1):19-23.
[9]Aouad MT,Nasr VG.Emergence agitation in children:an update[J].Curr OpinAnaesthesiol,2005,18(6):614-619.
[10]Arai YC,Fukunaga K,Hirota S.Comparison of a combination of midazolam and diazepam and midazolam alone as oral premedication on preanesthetic and emergence condition in children[J].ActaAnaesthesiol Scand,2005,49(5):698-701.
[11]Kim MS,Moon BE,Kim H,et al.Comparison of propofol and fentanyl administered at the end of anaesthesia for prevention of emergence agitation after sevoflurane anaesthesia in children[J].Br JAnaesth,2013,110(2):274-280.
[12]Kavalci G,Ethemoglu FB,Durukan P,et al.Comparison of the effects of dexmedetomidine and remiphentanyl on emergence agitation after sevoflurane anesthesia in adults undergoing septoplasty operation:a randomized double-blind trial[J]. Eur Rev Med Pharmacol Sci,2013,17(22):3019-3023.
[13]Salman AE,Camkiran A,Oguz S,et al.Gabapentin premedication for postoperative analgesia and emergence agitation after sevoflurane anesthesia in pediatric patients[J].Agri,2013, 25(4):163-168.
[14]Messieha Z.Prevention of sevoflurane delirium and agitation with propofol[J].Anesth Prog,2013,60(2):67-71.
[15]Ali MA,Abdellatif AA.Prevention of sevoflurane related emergence agitation in children undergoing adenotonsillectomy:A comparison of dexmedetomidine and propofol[J].Saudi JAnaesth,2013,7(3):296-300.
[16]Abdelhalim AA,Alarfaj AM.The effect of ketamine versus fentanyl on the incidence of emergence agitation after sevoflurane anesthesia in pediatric patients undergoing tonsillectomy with or without adenoidectomy[J].Saudi J Anaesth,2013,7 (4):392-398.
[17]Kanaya A,Kuratani N,Satoh D,et al.Lower incidence of emergence agitation in children after propofol anesthesia compared with sevoflurane:a meta-analysis of randomized controlled trials[J].JAnesth,2014,28(1):4-11.
[18]Kim YS,Chae YK,Choi YS,et al.A comparative study of emergence agitation between sevoflurane and propofol anesthesia in adults after closed reduction of nasal bone fracture[J]. Korean JAnesthesiol,2012,63(1):48-53.
[19]Yasui Y,Masaki E,Kato F.Sevoflurane directly excites locus coeruleus neurons of rats[J].Anesthesiology,2007,107(6): 992-1002.
Factors Related with Postoperative Agitation in Patients with Cerebral Palsy
LIU Hai-quan,WANG Zeng-chun,WANG Qiang,et al. Capital Medical University School of Rehabilitation Medicine,Department of Anesthesiology,Beijing Bo'ai Hospital,China Rehabilitation Research Center,Beijing 100068,China
ObjectiveTo explore the risk factors for postoperative agitation(PA)in patients with cerebral palsy(CP).Methods199 patients with CP receiving selective posterior rhizotomy or lower limbs orthopedics under combined intravenous and inhalational anesthesia were reviewed.Results30 patients suffered from PA(15%),who tended to be younger,less body mass,and administered less anesthetics.ConclusionIt may prevent PAof sufficient intra-operative and postoperative analgesia,necessary psychological intervention and sedatives.
cerebral palsy;postoperative agitation;pain
10.3969/j.issn.1006-9771.2014.05.005
R742.3
A
1006-9771(2014)05-0414-03
2013-11-13
2014-01-02)
1.首都醫科大學康復醫學院,北京市100068;2.中國康復研究中心北京博愛醫院麻醉科,北京市100068。作者簡介:劉海泉(1976-),男,河北廊坊市人,主治醫師,主要研究方向:臨床麻醉與疼痛。
猜你喜歡
環球時報(2022-12-23)2022-12-23 09:28:37
昆明醫科大學學報(2022年1期)2022-02-28 07:45:04
中老年保健(2021年11期)2021-08-22 03:13:36
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
河北畫報(2020年10期)2020-11-26 07:20:50
小學閱讀指南·低年級版(2017年1期)2017-03-13 20:07:35
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
中國醫療美容(2015年1期)2015-07-12 10:06:38
鄭州大學學報(醫學版)(2015年2期)2015-02-27 14:50:54
西南軍醫(2014年5期)2014-04-25 07:42:48