不同入路椎弓根釘棒內固定治療脊柱胸腰段骨折的臨床療效
2015-01-12 05:46:41呂志剛王廣超尚錦梁
中國現代醫生 2015年27期
關鍵詞:手術
呂志剛 王廣超 尚錦梁
河南省濟源市第二人民醫院骨科,河南濟源459000
不同入路椎弓根釘棒內固定治療脊柱胸腰段骨折的臨床療效
呂志剛 王廣超 尚錦梁
河南省濟源市第二人民醫院骨科,河南濟源459000
目的探討椎弓根釘棒不同入路方式內固定治療脊柱胸腰段骨折的臨床效果,為臨床選擇術式提供參考。方法回顧性分析2010年1月~2013年12月68例后路椎弓根釘棒內固定術式治療脊柱胸腰段骨折患者臨床資料,按術式分為正中入路組及Wiltse入路組,正中入路組34例患者實施傳統后正中入路手術,Wiltse入路組34例患者實施Wiltse入路手術。對比兩組患者臨床指標、影像學表現、肌酸激酶水平及疼痛評分。結果Wiltse入路組手術時間、出血量、引流量、住院時間均明顯低于正中入路組,差異均有統計學意義(P<0.05);Wiltse入路組術后1 d、3 d、5 d血清肌酸激酶水平均明顯低于正中入路組,差異均有統計學意義(P<0.05);兩組患者后凸Cobb角、傷椎前緣高度術后及末次隨訪相比術前兩組均有顯著改善(P<0.05),但兩組間術后及末次隨訪比較差異無統計學意義(P>0.05);Wiltse入路組術后1個月、術后6個月VAS評分分別為(2.05±0.41)、(0.69±0.12)分,均明顯低于正中入路組,差異均有統計學意義(P<0.05)。結論Wiltse入路椎弓根釘棒內固定治療與傳統入路方式治療骨折效果無明顯差異,但Wiltse入路治療胸腰段骨折操作簡便,創傷小,疼痛感低。
椎弓根釘棒;脊柱胸腰段骨折;Wiltse入路;內固定
椎體骨折以及腰椎退變常用手術治療,其中脊柱后路治療方式是主要術式,傳統后路術式顯露范圍大,對脊旁肌大范圍剝離和牽拉,導致頑固性腰背疼痛以及平背畸形等并發癥發生,嚴重影響患者生活質量[1,2]。近年來不同入路術式得以發展,其中Wiltse入路方式經椎旁肌間隙入路,對患者創傷更小。本文旨在探討椎弓根釘棒不同入路方式內固定治療脊柱胸腰段骨折的臨床效果,為臨床選擇術式提供參考,選擇68例脊柱胸腰段骨折患者,分別實施傳統入路及Wiltse入路,對比兩組患者術后表現,現將研究結果報道如下。
1 資料與方法
1.1 一般資料
回顧性分析2010年1月~2013年12月68例脊柱胸腰段骨折患者臨床資料,按手術方式分為正中入路組34例、Wiltse入路組34例。Wiltse入路組34例,男22例,女12例;年齡22~51歲,平均(36.92±6.21)歲;壓縮性骨折21例,爆裂性骨折13例;交通事故致傷19例,高處跌落致傷13例,其他致傷2例。正中入路組34例,男23例,女11例;年齡20~52歲,平均(36.58±6.55)歲;壓縮性骨折19例,爆裂性骨折15例;交通事故致傷17例,高處跌落致傷14例,其他致傷3例。兩組患者性別、年齡、骨折類型、致傷原因等基線資料比較差異無統計學意義(P>0.05),具有可比性。
1.2 納入標準
①患者均無需實施椎管減壓術;②骨折類型為單純爆裂性或壓縮性;③椎板、椎弓根、小關節結構完整[3,4];④無胸腰椎疾病史;⑤脊椎CT檢查證實患者為單節段骨折。
1.3 治療方法
(1)正中入路組:患者全麻,C臂機下定位骨折處,實施傳統后正中入路,確認多裂肌在棘突的起點,實施切斷,將骨膜下多裂肌剝離,直至關節突以及橫突位置處,確認人字嵴位置,此處進針,將椎弓根螺釘置入,并置入固定棒,復位后固定,逐層縫合。(2)Wiltse入路組:患者全麻,取俯臥位,C臂機下定位骨折端,確認腰背筋膜表面,實施皮下組織分離,直至正中旁約3 cm處,定位多裂肌及最長肌間隙,將肌間隙鈍性分離,并將小關節突外側電凝剝離,將椎弓根螺釘置入橫突基底部以及上關節突外緣中點處,并置入固定棒,復位后固定,逐層縫合。
1.4 觀察指標及評價標準
①臨床指標:手術時間、出血量、引流量、住院時間;②分別于術前、術后1 d、3 d、5 d檢測血清肌酸激酶水平;③影像學檢查:包括患者術前、術后Cobb's角、傷椎前緣高度;④術后1個月、6個月視覺模擬疼痛評分(VAS)[5,6]:在紙上面劃一條10 cm的橫線,橫線的一端為0,表示無痛;另一端為10,表示劇痛;中間部分表示不同程度的疼痛,讓病人根據自我感覺在橫線上劃一記號,表示疼痛的程度。
1.5 統計學方法
本文研究結果使用統計學軟件SPSS 21.0進行分析,計量資料以均數±標準差(±s)表示,采用t檢驗,不同時間點比較采用方差分析,P<0.05為差異有統計學意義。
2 結果
2.1 Wiltse入路組與正中入路組臨床指標比較
Wiltse入路組手術時間(54.38±11.32)min、出血量(160.43±38.49)mL、引流量(108.24±22.35)mL、住院時間(8.84±1.67)d均明顯低于正中入路組,差異均有統計學意義(P<0.01),見表1。
表1Wiltse入路組與正中入路組臨床指標比較(±s)

表1Wiltse入路組與正中入路組臨床指標比較(±s)
組別n手術時間(m i n)出血量(m L)引流量(m L)住院時間(d)W i l t s e入路組正中入路組t值P 3 4 3 4 5 4.3 8 ± 1 1.3 2 8 2.1 8 ± 1 8.4 5 7.4 8 9<0.0 1 1 6 0.4 3 ± 3 8.4 9 3 1 8.8 5 ± 5 2.1 6 1 4.2 5 0<0.0 1 1 0 8.2 4 ± 2 2.3 5 2 3 1.1 8 ± 3 0.5 7 1 8.9 3 0<0.0 1 8.8 4 ± 1.6 7 1 3.5 6 ± 2.4 7 9.2 3 1<0.0 1
2.2 Wiltse入路組與正中入路組血清肌酸激酶水平比較
Wiltse入路組與正中入路組術前血清肌酸激酶水平對比差異無統計學意義(P>0.05);Wiltse入路組術后1 d、3 d、5 d分別為(429.28±21.39)IU/L、(280.19± 14.43)IU/L、(181.55±12.37)IU/L,均明顯低于正中入路組,差異均有統計學意義(P<0.01),見表2。
2.3 Wiltse入路組與正中入路組影像學表現比較
兩組患者術前Cobb's角、傷椎前緣高度對比差異無統計學意義(P>0.05),術后及末次隨訪相比術前兩組均有顯著改善(P<0.05),但兩組間術后及末次隨訪比較差異無統計學意義(P>0.05),見表3。
2.4 兩組患者VAS評分比較
Wiltse入路組術后1個月、術后6個月VAS評分分別為(2.05±0.41)、(0.69±0.12),均明顯低于正中入路組,差異均有統計學意義(P<0.01),見表4。
表2Wiltse入路組與正中入路組血清肌酸激酶水平比較±s,IU/L)

表2Wiltse入路組與正中入路組血清肌酸激酶水平比較±s,IU/L)
組別n術前術后1 d術后3 d術后5 d F值P W i l t s e入路組正中入路組t值P 3 4 3 4 1 4 4.2 8 ± 1 1.2 4 1 4 9.5 2 ± 1 3.6 4 1.7 2 9>0.0 5 4 2 9.2 8 ± 2 1.3 9 8 2 4.2 9 ± 1 9.6 9 7 9.2 2 5<0.0 1 2 8 0.1 9 ± 1 4.4 3 5 5 3.5 3 ± 1 6.6 8 7 2.2 6 4<0.0 1 1 8 1.5 5 ± 1 2.3 7 2 6 2.3 8 ± 1 3.8 1 2 5.4 2 2<0.0 1 2 5.3 2 4 3 6.5 5 8<0.0 1<0.0 1
表3Wiltse入路組與正中入路組影像學表現比較(±s,n=34)

表3Wiltse入路組與正中入路組影像學表現比較(±s,n=34)
注:與術前對比,#P<0.05
組別時間C o b b ' s角(°)傷椎前緣高度(%)W i l t s e入路組正中入路組術前術后末次隨訪F值P術前術后末次隨訪F值P t組間末次隨訪P 4 9.8 9 ± 4.5 7 9 3.4 7 ± 6.2 7#9 2.6 1 ± 5.8 6#1 5.7 8<0.0 5 5 0.5 7 ± 4.6 7 9 4.6 8 ± 6.2 2#9 3.0 8 ± 5.2 5#1 4.1 1<0.0 5 0.8 1>0.0 5 1 9.5 8 ± 3.1 1 5.0 4 ± 1.1 6#6.5 9 ± 1.6 6#8.1 9<0.0 5 2 0.1 3 ± 3.3 7 4.8 6 ± 1.5 4#6.5 1 ± 1.0 7#8.6 9<0.0 5 0.4 6>0.0 5
表4 兩組患者VAS評分比較(±s)
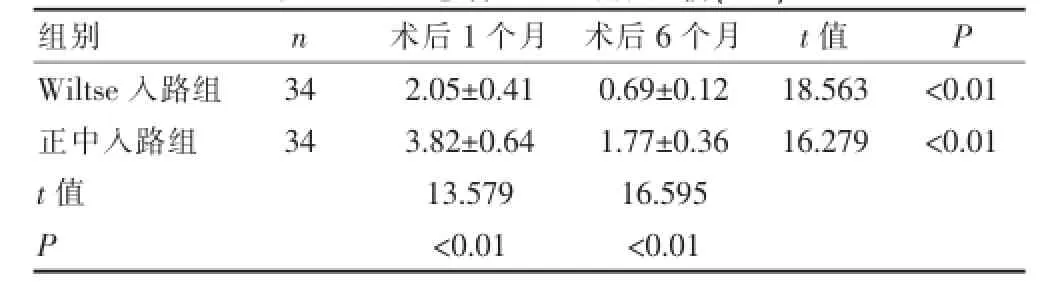
表4 兩組患者VAS評分比較(±s)
組別n術后1個月術后6個月t值P W i l t s e入路組正中入路組t值P 3 4 3 4 2.0 5 ± 0.4 1 3.8 2 ± 0.6 4 1 3.5 7 9<0.0 1 0.6 9 ± 0.1 2 1.7 7 ± 0.3 6 1 6.5 9 5<0.0 1 1 8.5 6 3 1 6.2 7 9<0.0 1<0.0 1
3 討論
目前治療脊柱胸腰段骨折手術主要目的是通過關節突完成置入內固定裝置物復位固定,傳統入路方式主要依靠大范圍剝離椎旁肌肉,因此對椎旁肌肉損傷很大,直接造成疼痛等并發癥。多裂肌是椎體棘突上部肌肉群,對脊柱活動主要起到定位作用[7,8],目前臨床公認腰神經后支是多裂肌的唯一支配神經,因此傳統正中入路對雙側多裂肌的大范圍剝離劑牽拉對肌肉機械性損害及神經的損傷均十分明顯。
本文結果顯示Wiltse術式手術時間更短,主要與術式特點有關,Wiltse術式通過正中切口向兩側分離直至肌間隙部位,通過經肌間隙分離,有利于醫生對患者上關節突定位,因此減短了暴露時間,有利于置入椎弓根螺釘實施固定,手術時間更短。同時Wiltse術式改善了傳統術式強行對椎旁肌肉剝離和牽拉的劣勢,肌間隙是利用最長肌以及多裂肌之間的間隙進入,因此無需剝離,保證了多裂肌深面神經支配[9-11]以及椎旁肌肉的損害,降低了術后疼痛,有利于術后快速恢復。本文研究結果顯示Wiltse術式患者術后VAS評分明顯較低,術后6個月僅(0.69±0.12)分,引流量也較少,住院時間更短,直接表明了Wiltse術式對患者肌肉及神經傷害更小,此外,血清肌酸激酶水平是反應肌肉損傷的直接標志物[12,13],本文血清肌酸激酶水平結果提示兩組患者治療后均有明顯提升,表明兩種術式均對肌肉有不同程度的損傷,但Wiltse術式血清肌酸激酶水平較傳統術式明顯更低,提示Wiltse術式對患者肌肉損傷更小。本文結果提示Wiltse術式患者術中出血量明顯更少,原因是Wiltse術式利用最長肌與多裂肌直接的間隙,所遇的血管更少,因此術中出血量少,對患者創傷小,這也是患者術后疼痛感更低的原因之一。此外,Wiltse術式對儀器、操作等無特殊要求,有利于在基層醫院推廣應用。本文對比傳統入路術式以及Wiltse術式治療差異,結果提示兩種入路手術治療效果相近,表明實質上以椎弓根釘棒為內固定物治療兩種術式均可以取得穩定的效果,抗骨質疏松藥物僅能起到促進術后恢復,加速骨折愈合的效果,骨折治療實質性效果仍取決于手術。在Wiltse術中,要快速準確定位多裂肌與最長肌的間隙,對于肥胖患者間隙距離正中旁較遠[14-15],對醫生判斷有所影響,因此建議有條件的醫院在術前實施橫斷位片對間隙定位,有利于術中快速準確完成手術。在利用C臂機過程中,可將手上椎體上下椎弓根體表的投影做標記,防止手術中發生固定節段錯誤。
綜上所述,Wiltse入路椎弓根釘棒內固定治療與傳統入路方式治療骨折效果無明顯差異,但Wiltse入路治療胸腰段骨折操作簡便,創傷小,疼痛感低,值得臨床推廣應用。
[1]鄭干軒,林慰光,胡奕山,等.前路與后路三維重建手術治療載荷分享評分≥7分的胸腰段骨折的效果比較[J].廣東醫學,2014,35(13):2084-2087.
[2]Fitzpatrick DC,Sheerin DV,WolfBR,et al.A randomized,prospective study comparing intertrochanteric hip fracture fixation with the dynamic hip screw and the dynamic helical hip system in a community practice[J].Iowa Orthop J,2011,31:166-172.
[3]唐謹,郭衛春,胡金鳳,等.后路椎弓根釘釘棒系統治療胸椎骨折27例的臨床療效[J].中華臨床醫師雜志(電子版),2011,5(18):5523-5526.
[4]Malley NT,Deeb AP,Bingham KW,et al.Outcome of the dynamic helical hip screw system for intertrochanteric hip fractures in the elderly patients[J].Geriatr Orthop Surg Rehabil,2012,3(2):68-73.
[5]文坤樹,蔣波,蔡勇平,等.椎弓根釘棒系統治療胸、腰椎骨折56例體會[J].重慶醫學,2012,41(15):1496-1499.
[6]Yeung M,Bhandari M.Uneven global distribution of randomized trials in hip fracture surgery[J].Acta Orthop,2012,83(4):328-333.
[7]何長街,劉志禮,舒勇,等.胸腰段骨折后外側融合后椎弓根釘棒系統斷裂原因分析[J].實用醫學雜志,2010,26(19):3593-3596.[8]Cheng T,Zhang G,Zhang X.Review:Minimally invasive versus conventional dynamic hip screw fixation in elderly patients with intertrochanteric fractures:A systematic review and meta-analysis[J].Surg Innov,2011,18(2):99-105.
[9]方向前,胡志軍,范順武,等.胸腰段骨折經肌間隙入路與傳統入路內固定的比較研究[J].中華骨科雜志,2009,29(4):315-318.
[10]Sahana H,Khajuria DK,Razdan R,et al.Improvement in bone properties by using risedronate adsorbed hydroxyapatite novel nanoparticle based formulation in a rat model of osteoporosis[J].Journal of Biomedical Nanotechnology,2013,9(2):193-201.
[11]丁健,唐亮,房宏生,等.椎弓根釘-棒結合椎體支柱塊治療胸腰椎骨折[J].實用骨科雜志,2011,17(9):773-775.
[12]Toyoaki Maruta,Go Otao,Takeshi Miyazato,et al.Effects of intravenous low-dose recombinant human atrial natriuretic peptide on renal function in the perioperative management for gastrointestinal perforation or ileus:A retrospective single-center study[J].J Crit Care,2013,28(2):133-140.
[13]胡華,蔣林,柳昊,等.PKP治療骨質疏松椎體壓縮性骨折術后椎體高度丟失的相關因素[J].中國老年學雜志,2014,34(13):3524-3526.
[14]Azar D,Mohsen J,Shila K.Effects of antenatal corticosteroids on maternal serum indicators of infection in women at risk for preterm delivery:A randomized trial com paring betamethasone and dexamethasone[J].Journal of research in medical sciences:the official journal of Isfahan University of Medical Sciences,2012,17(10):911-917.
[15]Eric D,Kristian T,Samantha H,et al.Interpreting discordant indirect and multiple treatment comparison metaanalyses:an evaluation of direct acting antivirals for chronic hepatitis C infection[J].Clinical Epidemiology,2013,5(5):173-183.
The clinical efficacy of different approaches of pedicle screw fixation in treatment of thoracolumbar fractures
LV ZhigangWANG GuangchaoSHANG Jinliang
Department of Orthopaedic,the Second People's Hospital of Jiyuan City in He’nan Province,Jiyuan459000,China
Objective To investigate clinical efficacy of different approaches of pedicle screw fixation in treatment of thoracolumbar fractures,to provide a reference for clinical surgery.Methods A retrospective analysis from January 2010 to December 2013 68 thoracolumbar fracture patients were performed,these patients were treated with posterior pedicle screw fixation rod,according to surgical approach they were divided into the middle group and Wiltse approach group,34 patients in midline approach groupused conventional surgical midline approach,Wiltse approach group 34 patients used embodiment Wiltse approach surgery.Clinical parameters between two groups of patients,imaging findings,creatine kinase levels and pain scores were compared.Results In Wiltse approach group,the operative time, blood loss,drainage,length of hospital stay were significantly lower than the control group,the differences were statistically significant(P<0.05);preoperative serum creatine kinase levels of Wiltse approach group showed no difference compared with control group(P>0.05),serum creatine kinase levels in Wiltse approach group 1 d,3 d,5 d after surgery were significantly lower than the control group,the differences were statistical significant(P<0.05);for two groups Cobb's angle,the leading edge of vertebral height both improved significantly(P<0.05),but at the time of the last follow-up,Cobb's angle and the leading edge of vertebral height between the two groups showed no significant difference (P>0.05);in Wiltse approach group after one month and after six months VAS scores were(2.05±0.41),(0.69±0.12) scores,significantly lower than the control group,the differences were statistically significant(P<0.05).Conclusion Wiltse approach pedicle screw fixation has same effect with the traditional way of treating fractures of thoracolumbar, but Wiltse approach is simple,less invasive,with low pain.
Pedicle screw;Thoracolumbar fractures;Wiltse approach;Fixation
R687.3
B
1673-9701(2015)27-0040-03
2015-06-01)
猜你喜歡
環球時報(2022-12-23)2022-12-23 09:28:37
昆明醫科大學學報(2022年1期)2022-02-28 07:45:04
中老年保健(2021年11期)2021-08-22 03:13:36
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
河北畫報(2020年10期)2020-11-26 07:20:50
小學閱讀指南·低年級版(2017年1期)2017-03-13 20:07:35
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
中國醫療美容(2015年1期)2015-07-12 10:06:38
鄭州大學學報(醫學版)(2015年2期)2015-02-27 14:50:54
西南軍醫(2014年5期)2014-04-25 07:42:48