秋冬季小兒呼吸道感染的病原學檢測及其分布特點分析
2016-12-10 03:17:04彭俊爭根廣州市婦女兒童醫療中心呼吸科廣東廣州510623
中國醫藥科學 2016年16期
彭俊爭 鄧 力 盧 根廣州市婦女兒童醫療中心呼吸科,廣東廣州 510623
秋冬季小兒呼吸道感染的病原學檢測及其分布特點分析
彭俊爭 鄧 力 盧 根▲
廣州市婦女兒童醫療中心呼吸科,廣東廣州 510623
目的 對秋冬季小兒呼吸道感染的非細菌性病原學檢測并對其分布特點進行分析,為臨床針對性治療提供參考依據。 方法 隨機選取廣州市婦女兒童醫療中心呼吸道感染患兒共1047例,并對其呼吸道分泌物和血清學進行病原學檢查,對結果進行統計分析。 結果 在1047例患兒血清病原學檢查中,單項感染326例,陽性率為31.14%,混合感染202例,陽性率為19.29%,單項感染比例明顯高于多項感染(P<0.05);在326例單項感染的患兒中,MP具有最高的陽性檢測率,為18.05%,其次為RSV(3.25%)、ADV(3.25%)、INFB(2.96%);在202例混合感染中,MP+INBF具有最高的陽性率,為10.32%,其次為MP+LP(2.77%),MP+LP+INBF(2.01%),MP+ADV(0.96%);6~12個月的患兒的陽性率(52.36%)明顯高于3~6個月患兒(P<0.05),1~3周歲患兒的陽性率(85.45%)明顯高于3~6個月患兒和6~12個月患兒(P<0.05)。在1047例患兒中經咽拭子病原學檢查發現,陽性患者為476例,陽性檢出率為45.46%。其中RSV具有最高的陽性檢測率,為19.87%,構成比為0.44,其次為RHV、RBOV、ADV;發現6~12個月的患兒的陽性率(48.21%)和構成比(0.40)均明顯高于3~6個月患兒(P<0.05),1~3周歲患兒的陽性率(75.45%)和構成比(0.52)均明顯高于3~6個月患兒和6~12個月患兒(P<0.05)。 結論 秋冬季我院呼吸道感染患兒以呼吸道合胞病毒、肺炎支原體感染為主,1~3歲患兒具有更高的陽性率。
兒科;呼吸道感染;病原學檢測,秋冬季
呼吸道感染一種臨床上最為常見的感染類型,常見的非細菌性呼吸道感有很多種,主要包括RSV、MP、ADV、FA、FB等[1-2]。呼吸道感染具有較為明顯的季節特征性[3],本次主要研究秋冬季小兒呼吸道感染非細菌性病原體的分布特點。
1 資料與方法
1.1 一般資料
隨機選取2014年9月~2015年2月于廣州市婦女兒童醫療中心就診并于呼吸科住院的呼吸道感染患兒1047例,男620例,女580例,年齡3個月~3周歲,平均1.6±0.7歲。其納入標準為:(1)年齡為3個月~3周歲;(2)病程小于等于5d;(3)發病后進行相關治療;(4)家屬簽署知情同意書。
1.2 分泌物標本測定
以上所有患兒均在入院后48h內進行標本采集,采集標本工具為小兒口咽拭子,患兒取坐或臥位,固定頭部,借助壓舌板暴露口咽部后將口咽拭子(華瑞安,批號:20140901)插入直達咽后壁,輕輕旋轉拭子,使咽后壁上的細胞及分泌物盡量粘附在拭子上,輕輕旋轉拭子并退出,采樣完畢后立即將試子放入無菌試管內,管內盛有2mL生理鹽水,測試或放入-80℃冰箱內保存待用。
將采集好的樣本從冷凍冰箱中取出,與4℃下融化后使用振蕩器充分搖勻,取200μL樣品置于1.5mL離心管中離心(Eppendorf),后進核酸提取,經逆轉錄后采用PCR擴增(西班牙Vircell. S.L公司),將擴增產物以及Alient Marker放置在全自動分析儀中(美國ABI公司),并使用QI Axcel BioCaculator軟件進行分析。
1.3 血液樣本測定
將所有患兒均抽取靜脈血4mL,于3000/rpm轉速離心10min,將上層血清樣品放入-20℃的冰箱保存,采用血清特異性IgM抗體的定性,使用熒光顯微鏡(奧林巴斯熒光顯微鏡型號BX51,試劑批號201409-201502)測定。
1.4 統計學方法
本次研究使用SPSS18.0 軟件進行分析,計數資料用率(%)來表示,采用χ2檢驗,當P<0.05時表示差異具有統計學意義。
2 結果
2.1 血清學病原結果
2.1.1 一般結果 本次研究共有呼吸道感染患兒1047例,其中單項感染326例,陽性率為31.14%,構成比為0.62,混合感染202例,陽性率為19.29%,構成比為0.38。單項感染比例明顯高于多項感染(χ2= 6.28, P<0.05),其具體數值見表1。

表1 病原體總檢出率[n(%)]
2.1.2 9種小兒呼吸道病原體單項感染檢出情況 在362例單項感染的患兒中,MP具有最高的陽性檢測率為18.5%(189例),構成比為0.58,其次分別為RSV(3.25%)、ADV(3.25%)、INFB(2.96%),其具體數值見表2。

表2 單項感染檢出情況[n(%)]
2.1.3 小兒呼吸道病原體混合感染檢出情況 在202例混合感染中,MP+INBF具有最高的陽性率,為10.32%,構成比為0.53,其次為MP+LP(2.77%),MP+LP+INBF(2.01%),MP+ADV(0.96%),其具體陽性率和構成比見表3。
2.1.4 9種小兒呼吸道病原體感染在不同年齡段總體檢出情況 對1047例患兒根據年齡分為3組,發現6~12個月的患兒的陽性率(52.36%)和構成比(0.39)均明顯高于3~6個月患兒(P<0.05),1~3周歲患兒的陽性率和構成比均明顯高于3~6個月患兒和6~12個月患兒(P<0.05)。見表4。
2.2 咽拭子病原學結果
2.2.1 11種小兒呼吸道病原體單項感染檢出情況 本次研究共有呼吸道感染患兒1047例,其中陽性患者為476例,陽性檢出率為45.46%。其中RSV具有最高的陽性檢測率,為19.87%,構成比為0.44,其次為RHV、RBOV、ADV,其具體陽性率和構成比見表5。
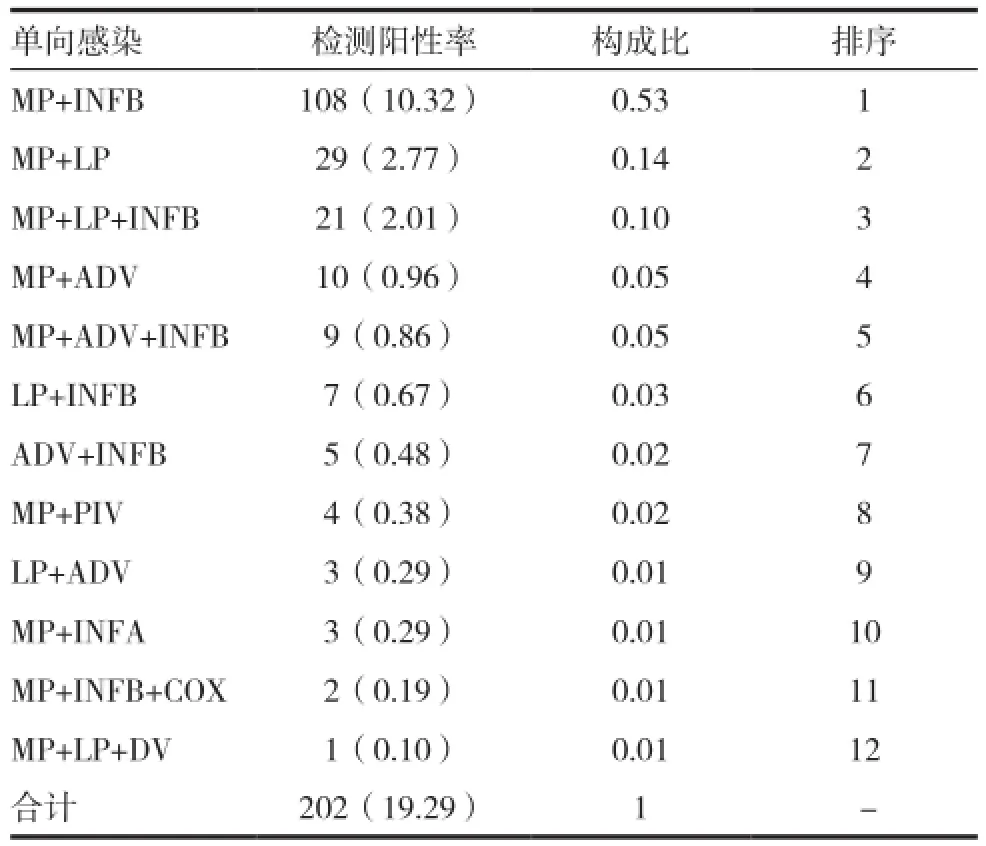
表3 混合感染檢出情況[n(%)]

表4 不同年齡段總體感染情況[n(%)]

表5 單項感染檢出情況[n(%)]
2.2.2 不同年齡段11種病原體總體檢出情況 對1047例患兒根據年齡分為3組,發現6~12個月的患兒的陽性率(48.21%)和構成比(0.40)均明顯高于3~6個月患兒(P<0.05),1~3周歲患兒的陽性率(75.45%)和構成比(0.52)均明顯高于3~6個月患兒和6~12個月患兒(P<0.05)。

表6 不同年齡段總體感染情況[n(%)]
3 討論
呼吸道感染可分為上呼吸道感染和下呼吸道感染,呼吸道感染具有傳播快、流行廣等特點[4-5],并且在兒童群體具有很高的感染率,兒童每年發生呼吸道感染的次數可高達6~8次,并且小兒呼吸道感染具有病情發生急速、進展快、病程長等特點[6-7],還容易引起其他系統和器官的損傷,是導致5歲以下兒童死亡的第二大病因[8-9]。近年來的研究表明,我國每年兒童呼吸道感染超過1.3億人次,每年死于呼吸道感染的兒童高達200萬例[10-12]。能夠引起呼吸道感染的病原體包括細菌、病毒和非典型病原體三種[13],由于近年來由于抗生素的大量使用使得細菌感染率有所降低而非典型病原體的比例有所增加,而對病毒性感染尚無特異性治療[14-16]。本研究通過對秋冬季小兒呼吸道感染的非細菌性病原學檢測并對其分布特點進行分析可為臨床針對性治療提供參考依據。
本次研究共有呼吸道感染患兒1047例,經血清學病原檢查發現,單項感染326例,陽性率為31.14%,構成比為0.62,混合感染202例,陽性率為19.29%,構成比為0.38,單項感染比例明顯高于多項感染(P<0.05);在單項感染中,MP具有最高的陽性檢測率為18.5%(189例),其次分別為RSV、ADV、INFB;在202例混合感染中,MP+INBF具有最高的陽性率,為10.32%,構成比為0.53,其次為MP+LP,MP+LP+INBF,MP+ADV;發現6~12個月的患兒的陽性率(53.31%)和構成比(0.40)均明顯高于3~6個月患兒(P<0.05),1~3周歲患兒的陽性率(85.45%)和構成比(0.53)均明顯高于3~6個月患兒和6~12個月患兒(P<0.05)。經咽拭子病原學檢查發現,陽性患者為476例,陽性檢出率為45.46%。其中RSV具有最高的陽性檢測率,為19.87%,構成比為0.44,其次為RHV、RBOV、ADV;發現6~12個月的患兒的陽性率(48.21%)和構成比(0.40)均明顯高于3~6個月患兒(P<0.05),1~3周歲患兒的陽性率(75.45%)
和構成比(0.52)均明顯高于3~6個月患兒和6~12個月患兒(P<0.05)。通過本次研究發現小兒呼吸道非細菌性感染以RSV為主,其次以MP為主,并且呼吸道感染的檢出率與年齡密切相關,3周歲以下患兒隨著年齡的增加陽性率也隨著增加。本次研究為呼吸道感染的病原學及其檢測積累了檢測經驗及數據,為進行科學有效的小兒呼吸道感染的預防控制提供實驗室依據。
[1] van Woensel JB, van Aalderen WM, Kimpen JL. Vral lower respiratory tract infection in infants and young children[J]. BMJ,2003,327(7405): 36-40.
[2] Nair H, Nokes DJ, Gessner BD, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysisp[J].Lancet,2010, 375(9725): 1545-1555.
[3] 周一平. 成人急性下呼吸道感染患者病毒病原學研究[J]. 中國呼吸與危重監護雜志, 2010,9 (4): 379-382.
[4] Moore HC,de Klerk N,Richmond P,et a1.A retrospective population-based cohort study identifying target areas for prevention of acute lower respiratory infections in children[J]. BMC Public Health,2010,(10)10: 757.
[5] 謝紅梅. 1647例呼吸道感染病原體的IgM體檢測結果分析[J]. 中華醫院感染學雜志,2012, 22(12) :2696-2698.
[6] 肖愛蓮. 呼吸道1gM九聯檢臨床觀察240例分析[J].衛生職業教,2013, 31(14): 147-148.
[7] Choi IS, Byeon JH, Yoo Y, et al. Increased serum interleukin-5 and vascular endothelial growth factor in children with actue Mycoplasma pnermoniae and wheeze [J]. Pediatr Pulmonol, 2009, 44(5): 423-428.
[8] 周新華.呼吸道感染患兒病原學及血常規檢測的價值意義[J]. 中國醫學工程,2012, 20(1): 120-121.
[9] Nair H, Nokes DJ, Gessner BD, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: asystematic review and meta-analvsis[J].Lancet,2010,375(97251): 1545-1555.
[10] Rodriguez-Auad JP, Nava-Frias M, Casasola-Flares J,et al. The epidemiology and clinical characteristics of respiratory syncytial virus infection in children at a public pediatric referral hospital in Mexico [J]. Int J Infect Dis,2012,16(7):e508-e513.
[11] 江麗.福州地區4060例呼吸道感染患者病原體檢測結果分析[J]. 檢驗醫學與臨床,2014,11(4): 483-484.
[12] Semple Mq Taylor-Robinson DC, Lane S, et al. Household smoke and admission weight predict severe bronchiolitis in infant independent of deprivation:prospective cohort study[J]. PLoS One, 2011, 6(7):e224-225.
[13] 張在亭. 急性呼吸道感染住院小兒的多病原聯合檢測分析[J]. 中華臨床醫師雜志(電子版),2012,6(12):3408-3410.
[14] Johnson JI, Ratard R.Respiratory syncytial virusassociated hospitalizations in Louisiana [J]. J La State Med Soc,2012, 1640(5): 268-273.
[15] 胡偉.9項呼吸道病原體檢測在呼吸道感染病因分析中的應用[J]. 國際檢驗醫學雜志,2013, 34(23):3158-3161.
[16] 趙延香.小兒肺炎的細菌學耐藥性分析與檢驗質量控制[J].中國醫學創新,2015,12(31):124-127.
Pathogenic detection of respiratory infection in children in autumn and winter and its distribution characteristics
PENG Junzheng1DENG Li1LU Gen2
1. Department of Respiration, Women and Children Medical Center, Guangzhou 510623, China
Objective To analyze the non-bacterial pathogen detection in children in autumn and winter and its distribution characteristics. Methods 1047 cases of respiratory tract infection in children were randomly selected from women and children medical center. Its respiratory secretions and serum were detected, and its results were statistically analyzed. Results In 1047 respiratory infection samples, there were 326 cases with single infection, and the positive rate was 31.14%. There were 202 cases with mixed infection, and the positive rate was 19.29%. The single infection rate was significantly higher than mixed infection rate (P<0.05). In the 326 cases of single infection, MP had the highest positive detection rate with 18.05%, followed by RSV (3.25%), ADV (3.25%), and INFB (2.96%). In the 202 cases of mixed infection, MP+INBF had the highest positive detection rate with 10.32%, followed by MP+LP (2.77%), MP+LP+INBF (2.01%),MP+ADV (0.96%). Positive rate of 6-12 months of children (52.36%) was significantly higher than that of 3-6 months of children (P<0.05). Positive rate of 1-3 years of children (85.45%) was significantly higher than that of 3-6 months of children and 6-12 months of children (P<0.05). In the 1047 cases of respiratory infection samples, etiological examination of the pharyngeal swab showed that positive patients were 476 cases, and the positive detection rate was 45.46%. Among them, RSV had the highest positive detection rate with 19.87%, the proportion was 0.44, followed by RHV, RBOV, ADV. Positive rate (48.21%) of children in 6-12 months and composition ratio (0.40) were significantly higher than those of children in 3-6 months (P<0.05). Positive rate (75.45%) of children in 1-3 years and composition ratio (0.52) were significantly higher than those of children in 3-6 months and 6-12 months (P<0.05). Conclusion For respiratory tract infection in children in autumn and winter of our hospital, respiratory tract infection and mycoplasma pneumoniae infection are the most common. It had a higher positive rate for children in 1-3 years.
Pediatrics; Respiratory tract infection; Pathogen detection; Autumn and winter
R446.5
B
2095-0616(2016)18-21-04
2016-08-09)
▲通訊作者
猜你喜歡
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
幽默大師(2020年11期)2020-11-26 06:12:18
幽默大師(2020年10期)2020-11-10 09:07:20
海峽姐妹(2019年12期)2020-01-14 03:24:46
電子制作(2018年18期)2018-11-14 01:48:24
山東工業技術(2016年15期)2016-12-01 05:31:22
海峽科技與產業(2016年3期)2016-05-17 04:32:12
