老年患者脊柱術后發生急性精神障礙的相關因素分析
2017-05-18 08:17:03龍新華周云飛杜瀏學陳海鳴南昌大學第一附屬醫院急診外科骨科江西南昌330006
轉化醫學電子雜志 2017年4期
龍新華,周云飛,杜瀏學,陳海鳴(南昌大學第一附屬醫院:急診外科,骨科,江西南昌330006)
·臨床與轉化醫學·
老年患者脊柱術后發生急性精神障礙的相關因素分析
龍新華1,周云飛2,杜瀏學2,陳海鳴1(南昌大學第一附屬醫院:1急診外科,2骨科,江西南昌330006)
目的:探討老年患者脊柱手術后發生急性精神障礙(POP)可能的原因,以便指導臨床預防.方法:收集2010-01-01/2016-01-01在南昌大學第一附屬醫院行脊柱手術的65歲以上患者臨床資料,分析出現術后精神障礙(A組)與未出現術后精神障礙(B組)患者性別、基礎疾病、酗酒史、手術持續時間、術中出血、術后血清白蛋白、電解質水平以及手術節段與術后精神障礙的關系.結果:共收集患者4030例,其中出現術后精神障礙者180例,發生率為4.46%.男性發病率高于女性.A組患者中有酗酒史、高血壓病史、糖尿病病史、手術持續時間>3 h、術中出血>500 mL、術后低蛋白血癥以及低鈉、低鉀血癥發生率顯著高于B組.頸、胸、腰不同手術節段手術之間POP發生率無明顯差異(P=0.138).但是頸椎不同手術方式之間POP發生率存在顯著差異(P<0.001).Logistic回歸分析結果提示:酗酒史、高血壓病史、糖尿病病史、手術時間、低白蛋白血癥、電解質紊亂為老年患者脊柱術后精神障礙可能的危險因素.結論:本研究分析并提出老年患者脊柱術后精神障礙發生的可能危險因素為臨床預見性實施干預措施,有效預防術后精神障礙的發生或避免其導致的不良后果提供參考.但POP發病確切的高危因素需在多中心、多因素回顧性研究以及前瞻性研究中進一步發現和證實.
術后精神障礙;危險因素;脊柱手術
0 引言
脊柱手術一般在全身麻醉下完成,術后需要一定時間的臥床休息.在臨床工作中發現,許多患者在手術后出現譫妄、定向力障礙、躁動、煩躁不安、神智不清、嗜睡、胡言亂語、晝夜顛倒等精神障礙表現,且其中絕大多數為老年患者.術后精神障礙(postoperative psychonosema,POP)表現譫妄者居多,一般發生于術后15 d[1],雖然患者精神癥狀多能在約1周后自行緩解或者運用小劑量抗精神異常藥物后完全緩解,但這一時期恰好與脊柱術后需要嚴格臥床休息配合治療的時期重疊,患者術后精神障礙不能很好地配合治療以及功能鍛煉,增加了術后護理難度,使術后并發癥的發生率大大提高,嚴重影響手術效果及患者生活質量.因此預防老年患者脊柱術后精神障礙發生對減少術后并發癥,提高手術療效以及患者生活質量至關重要.本研究通過對2010-01-01/2016-01-01在南昌大學第一附屬醫院接受脊柱手術并發生術后精神障礙的老年患者臨床資料進行回顧性分析,擬尋找老年患者脊柱術后發生精神障礙的可能相關因素,并通過Logistic回歸分析探討出現術后精神障礙的高危因素,為臨床中預防老年患者脊柱術后精神障礙的發生提供參考.
1 資料和方法
1.1 一般資料收集2010-01-01/2016-01-01在南昌大學第一附屬醫院行脊柱手術的65歲及以上患者的臨床資料,回顧性分析出現術后精神障礙(A組)與未出現術后精神障礙(B組)患者性別、基礎疾病、酗酒史、手術持續時間、術中出血、術后血清白蛋白、電解質水平以及脊柱手術節段等臨床資料與術后精神障礙的關系.
1.2 排除標準患者有精神病病史或者家族史、術前存在精神障礙以及術后通過CT或者MRI檢查提示存在器質性病變的病例不納入本研究.
1.3 納入標準術后精神障礙診斷標準參照美國精神病學會1987年診斷標準:(1)對環境的意識減退且有轉移,集中和保持環境刺激的注意力下降.(2)至少出現以下2條:①知覺障礙;②語言不連貫;③睡眠清醒節律失調;④神經運動性活動減少.(3)定向失調和記憶減退.(4)臨床表現持續數小時、數日,有時1 d內晝夜有波動.
1.4 統計學處理所有數據應用SPSS13.0統計學軟件進行分析,計數資料采用χ2檢驗;將單因素分析結果中P<0.05的因素進行多因素Logistic回歸分析,以P<0.05為差異有統計學意義.
2 結果
2.1 老年患者脊柱術后精神障礙相關因素的單因素分析老年患者脊柱術后精神障礙的發生與性別、酗酒史、高血壓病史、糖尿病病史、手術時間、低白蛋白血癥、低鈉、低鉀血癥等因素有一定的相關性,差異有統計學意義(P<0.05).頸、胸、腰不同手術節段手術之間POP發生率比較,差異無統計學意義(P=0.138).但是頸椎不同手術方式之間POP發生率比較,差異有統計學意義(P<0.001,表1).
2.2 影響老年患者脊柱術后精神障礙的多因素Logistic回歸分析結果篩選出發生術后精神障礙的可能高危因素有:酗酒史、高血壓病史、糖尿病病史、手術時間長、術中出血多、低白蛋白血癥、低鈉、低鉀血癥(表2).
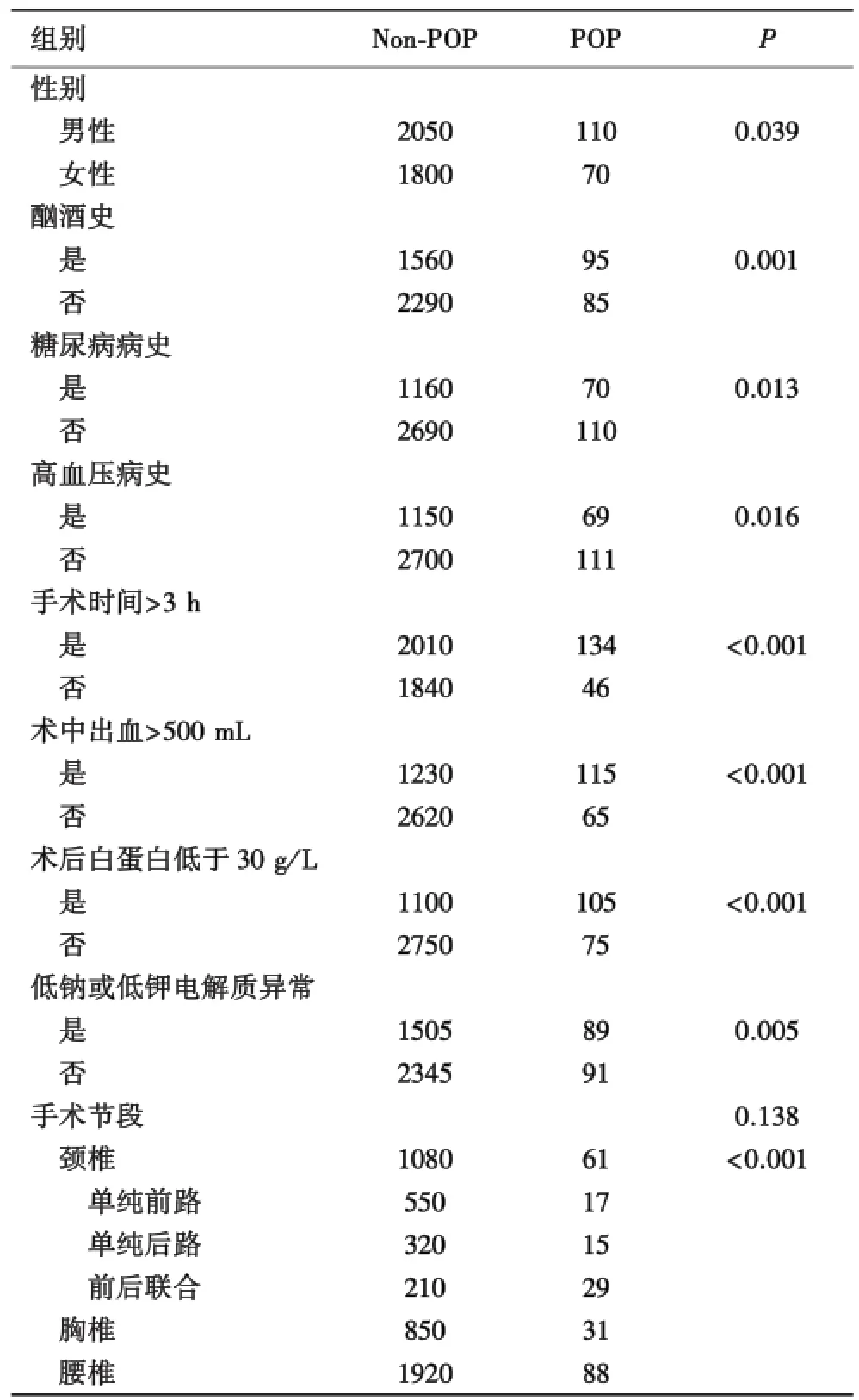
表1 老年患者脊柱術后精神障礙相關因素的單因素分析
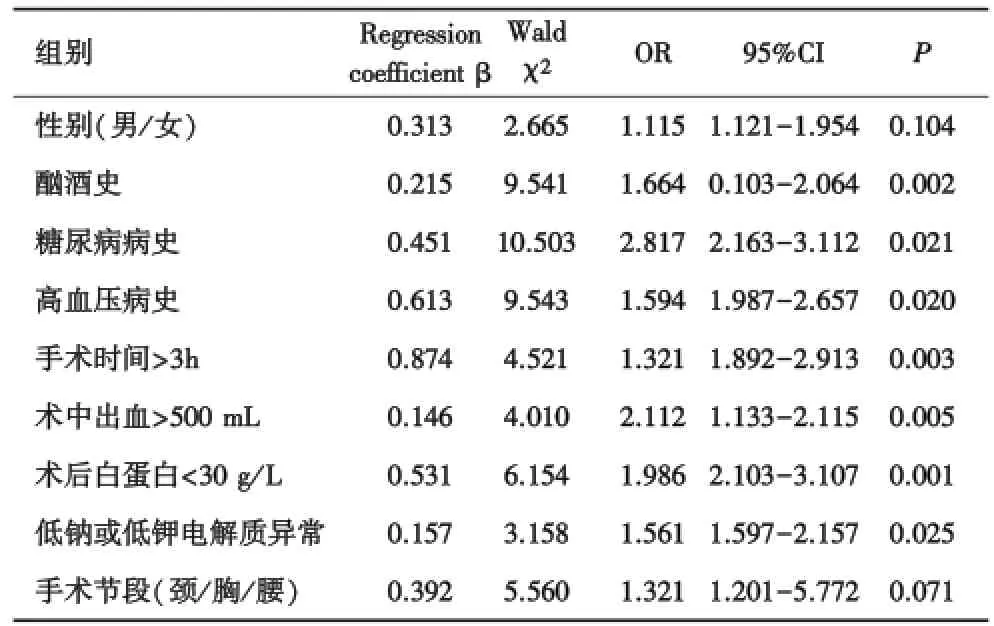
表2 影響老年患者脊柱術后精神障礙的多因素Logistic回歸分析
3 討論
術后精神障礙(postoperative psychonosema,POP)是指術前沒有精神異常的患者受圍術期各種因素的影響,術后數天內出現的腦功能暫時性功能障礙的一種可逆的、具有波動性的急性精神紊亂綜合征[2].POP主要臨床表現包括焦慮、譫妄、幻覺、躁狂、抑郁等,其中最為多見的表現為譫妄.手術后精神障礙多發生于術后1~5 d,尤以老年患者居多[3].關于術后精神障礙發生的機制尚不明確,曾經有學者相繼提出細胞代謝水平學說、神經遞質學說、應激反應學說及睡眠覺醒障礙學說等理論假說[4-6],每個假說都有其科學性,但都難以全面解釋術后精神障礙的發生.最近,Sousa等研究發現術后精神障礙與酗酒史密切相關[7].還有學者最新研究發現,術中低血氧以及低血壓易導致術后精神障礙[8-9].很顯然,術后精神障礙的發生是多因素、多水平作用的結果.近年來,越來越多的老年人接受脊柱手術,臨床中脊柱術后精神障礙的發生也較為常見.因大多脊柱術后患者需要臥床休息并在醫師指導下行功能鍛煉,POP的發生大大增加了護理難度及工作量,增加了術后并發癥及病死率,延長了住院時間,同時延遲了患者的康復.因此尋找和分析POP發生的高危因素對臨床上采取相應預防措施至關重要.本研究對南昌大學第一附屬醫院脊柱術后老年患者進行大樣本回顧性分析,尋找老年患者脊柱術后發生精神障礙的可能相關因素及高危因素,為臨床預防脊柱術后POP提供參考.
本研究結果顯示:4030例脊柱手術后老年患者中有180例發生術后精神障礙,其中男110例,女70例,頸椎手術1141例(61例POP),胸椎手術881例(31例POP),腰椎手術2008例(88例POP),不同手術節段之間POP發生率無明顯差異(P=0.138).本研究對頸椎手術不同手術方式進一步分析發現:單純前路手術有567例(17例POP)、單純后路手術335例(15例POP)、前后聯合手術239例(29例POP),他們之間POP發生率存在顯著差異(P<0.001),這可能與頸椎前路手術時間短、出血少、對患者全身情況影響小等因素有關.另外,患者中有酗酒史者更容易出現術后精神障礙,這與許多研究結果不謀而合[7,10-11].但是男性比女性更容易發病,與Shi等[12]和Fineberg等[13]的研究結果不同,這可能與國內男性酗酒者更多有關.此外,手術時間越長,術中出血越多,術后越容易出現精神障礙.術后患者低蛋白血癥以及電解質紊亂不僅關系到POP發病,而且關系到術后POP持續時間以及嚴重程度.術后有效處理低蛋白血癥,糾正電解質紊亂有利于精神障礙癥狀緩解,縮短持續時間,并預防進一步加重,是處理術后精神障礙的基本條件.另外,必要的心理輔導及家屬的盡心照顧也有利于預防POP發生以及已有癥狀的盡快緩解.
綜上所述,性別、酗酒史、高血壓病史、糖尿病病史、手術時間、術中出血量、術后白蛋白水平及電解質水平均為老年患者脊柱術后精神障礙發生的可能相關因素,其中酗酒史、高血壓病史、糖尿病病史、手術時間長、術中出血多、低白蛋白血癥、低鈉、低鉀血癥為POP的高危因素.雖然本研究所含樣本量較大,但是所有病例均來自南昌大學第一附屬醫院,為單中心、回顧性研究,其中部分病例資料存在不確切性并難以回訪考證,POP發病確切的高危因素將在下一步多中心、多因素回顧性研究以及前瞻性研究中進一步發現和證實.
[1]Sanders RD,Coburn M,Cunningham C,et al.Risk factors for post?operative delirium[J].Lancet Psychiatry,2014,1(6):404-406.
[2]Youngblom E,DePalma G,Sands L,et al.The temporal relation?ship between early postoperative delirium and postoperative cognitive dysfunction in older patients:a prospective cohort study[J].Can J Anaesth,2014,61(12):1084-1092.
[3]Yonekura H,Hirate H,Sobue K.Incidence,Risk Factors,and Effects on Outcome of Postoperative Delirium in Patients Undergoing Esophagectomy[J].Masui,2015,64(6):597-602.
[4]Witlox J,Eurelings LS,de Jonghe JF,et al.Delirium in elderly patients and the risk of postdischarge mortality,institutionalization,and dementia:a meta?analysis[J].JAMA,2010,304(4):443-451.
[5]Alvarez Fernandez B,Formiga F,Gomezr R.Delirium in hospitalised older persons:Review[J].J Nutr Health Aging,2008,12(4):246-251.
[6]Martin BJ,Buth KJ,Arora RC,et al.Delirium:a cause for concern beyond the immediate postoperative period[J].Ann Thorac Surg,2012,93(4):1114-1120.
[7]Sousa G,Pinho C,Santos A,et al.Postoperative delirium in patients with history of alcohol abuse[J].Rev Esp Anestesiol Reanim,2016:S0034-9356(16)30092-5.
[8]Soh S,Shim JK,Song JW,et al.Postoperative delirium in elderly patients undergoing major spinal surgery:role of cerebral oximetry[J].J Neurosurg Anesthesiol,2016.
[9]Kappen TH,Wesselink EM,van Klei WA,et al.Intraoperative hypotension and postoperative delirium:no confusion on confounding[J].Br J Anaesth,2016,116(6):887-888.
[10]Novakovic M,Dejanovic SD,Maric?Burmazevic J,et al.Alcoholic and postoperative delirium:a case?control study[J].Psychiatr Danub,2015,27(1):90-96.
[11]Gvozdenovic L,Antanaskovic A.History of alcohol abuse after major non?cardiac surgery and postoperative cognitive dysfunction[J].Eur J Intern Med,2015,26(9):e51.
[12]Shi C,Yang C,Gao R,et al.Risk Factors for Delirium After Spinal Surgery:A Meta?Analysis[J].World Neurosurg,2015,84(5):1466-1472.
[13]Fineberg SJ,Nandyala SV,Marquez?Lara A,et al.Incidence and risk factors for postoperative delirium after lumbar spine surgery[J].Spine,2013,38(20):1790-1796.
Analysis of risk factors for acute postopera?tive psychonosema in the elderly patients after spinal surgery
LONG Xin?Hua1,ZHOU Yun?Fei2,DU Liu?Xue2,CHEN Hai?Ming11Department of Emergency Surgery,2Department of Orthopedics,the First Affiliated Hospital of Nanchang University,Nanchang 330006,China
AIM:To explore the causes of high risk for the acute postoperative psychonosema(POP)of the elderly after spinal surgery and in order to guidw clinical prevention.METHODS:Elderly patients(above 65 years)who underwent spinal surgery at the First Affiliated Hospital of Nanchang University from Janu?ary 2010 to January 2016 were retrospectively reviewed.Patients with(group A)or without(group B)POP and related parame?ters,such as gender,underlying disease,alcohol history,dura?tion of surgery,intraoperative bleeding,postoperative serum albu?min,electrolyte levels and surgical segment et al,were collected and analyzed.The study was approved by the ethical research committee.RESULTS:A total of 180 of 4030 patients(4.46%)occurred POP.Incidence in males was higher than that in females.Patients who have history of alcohol,hypertension,diabetes mel?litus,duration of operation more than 3 hours,intraoperative bleeding greater than 500 mL,postoperative hypoproteinemia and hyponatremia,hypokalemia were higher than those of Group B.There was no statiatically significant on the incidence rate of POP among various surgical segments(P=0.138),but there was sig?nificant differences among different surgical procedure of cervical,chest and waist(P<0.001).Logistic regression suggested that alcohol history,duration of surgery,intraoperative bleeding,post?operative serum albumin,and electrolyte levels were risk factors of acute PoP in the elderly patients.CONCLUSION:The study reveals the possible risk factors of POP in the elderly patients with spine surgery,which provids reference for the prevention of POP.However,the exact risk factors for the incidence of POP still need to be further identified and confirmed by multicenter,multivari?ate,retrospective,and prospective studies.
postoperative psychonosema;risk factors;spinal surgery
R749.1+6
B
2095?6894(2017)04?31?03
2016-11-18;接受日期:2016-11-05
龍新華.E?mail:chenhaiming2797@126.com
陳海鳴.E?mail:chenhaiming2797@126.com
猜你喜歡
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
河北畫報(2020年10期)2020-11-26 07:20:50
電子制作(2018年18期)2018-11-14 01:48:24
山東工業技術(2016年15期)2016-12-01 05:31:22
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
中國中醫藥現代遠程教育(2014年11期)2014-08-08 13:23:44
西南軍醫(2014年5期)2014-04-25 07:42:48
中國中醫藥現代遠程教育(2014年13期)2014-03-01 04:26:36
終身教育研究(2014年5期)2014-02-28 01:23:06
