激光汽化術與前列腺電切術治療良性前列腺增生療效的Meta分析*
2017-08-22 04:23:27張曉波陳明泉陳雄戴元清齊觀南董超白耀譚新驥谷杰胡勝李東杰
中國內鏡雜志 2017年7期
張曉波,陳明泉,陳雄,戴元清,齊觀南,董超,白耀,譚新驥,谷杰,胡勝,李東杰
(中南大學湘雅醫院國際醫療部 外科,湖南 長沙 410008)
激光汽化術與前列腺電切術治療良性前列腺增生療效的Meta分析*
張曉波,陳明泉,陳雄,戴元清,齊觀南,董超,白耀,譚新驥,谷杰,胡勝,李東杰
(中南大學湘雅醫院國際醫療部 外科,湖南 長沙 410008)
目的 系統評價經尿道980nm激光汽化術與前列腺電切術(TURP)治療良性前列腺增生(BPH)的療效。方法收集國內外關于經尿道980nm激光汽化術與TURP治療BPH的文獻,采用Revman 5.3軟件進行Meta分析。結果篩選后共6篇文獻符合納入標準,總計839例,其中包括980nm激光治療組450例和TURP組389例。Meta結果顯示:和TURP組相比,980nm激光組手術時間差異無統計學意義[標準化均數差(SMD)=0.11,95%CI(-0.52,0.74),P >0.05],住院時間較短 [SMD=-1.95,95%CI(-3.42,-0.48),P <0.05]及術后尿管留置時間較短 [SMD=-2.64,95%CI(-3.92,-1.36),P <0.05]。980 nm 激光組和TURP組在術后國際前列腺癥狀評分(IPSS)差異無統計學意義[加權均數差(WMD)=0.12,95%CI(-0.27,0.51),P >0.05],術后生活質量評分(QOL)評分差異無統計學意義[SMD=0.00,95%CI(-0.57,0.57),P >0.05],術后最大尿流率(Qmax)差異無統計學意義 [SMD=0.06,95%CI(-0.26,0.37),P >0.05]。結論980nm激光治療良性BPH與經典的TURP術式相比,在住院時間和術后尿管留置時間方面有優勢,遠期效果無明顯差異。
良性前列腺增生;經尿道980nm激光汽化術;經尿道前列腺電切術
良性前列腺增生(benign prostate hyperplasia,BPH)是引起中老年男性排尿障礙的常見疾病,隨著年齡的增長,其發病率逐漸增加[1-2]。經尿道前列腺電切術(transurethral resesction of prostate,TURP)是目前BPH治療的金標準[3],但它仍存在如術中出血較多,易并發經尿道電切綜合征等不足,且其對高齡或合并其他嚴重疾病的患者并不合適[4]。經尿道980nm激光前列腺汽化術是治療BPH的新方法,它具有優秀的組織消融和止血能力[5]。本研究收集整理了國內外對上述兩種手術方式進行對比的相關臨床研究,并按Cochrane標準進行Meta分析,以期為臨床提供參考。
1 資料和方法
1.1 檢索方式
系統檢索了中國知網、萬方、維普cqvip、中國生物文獻數據庫(CBMdisc)、Pubmed、Embase、OVID和Cochrane等中英文數據庫,以980nm激光、TURP和BPH等檢索詞進行檢索,收集了公開發表的相關文獻。
中文檢索詞:980nm激光,半導體激光,經尿道前列腺電切術,前列腺增生;英文檢索詞:980 nm laser,diode laser,transurethral resection,TURP,prostatic hyperplasia,BPH。
1.2 納入標準
①研究類型:比較980nm激光治療和TURP治療BPH的研究;②研究對象:診斷明確且需要手術治療的BPH患者;③干預措施:實驗組采用經尿道980 nm激光治療,對照組采用TURP治療;④評價指標:包括安全性指標和有效性指標,其中安全性指標包括住院時間、手術時間和留置導尿管時間,有效性指標包括國際前列腺癥狀評分(international prostate symptom score,IPSS)、術后生活質量評分(the quality of life,QOL)和 最 大 尿 流 率(maximum flow rate,Qmax);⑤文獻時間:數據庫建立至2017年4月30日。
1.3 排除標準
①診斷不明確,不能排除前列腺癌、前列腺炎等疾病;②合并神經源性膀胱、嚴重尿路感染等疾病;③不符合手術指征或者不耐受手術者。
1.4 納入研究質量評分
參照改良Jadad標準對納入的研究進行方法學質量評分[6],包括隨機序列的產生、隨機化隱藏、盲法和失訪退出等。1~3分視為低質量研究,4~7分視為高質量研究。
1.5 統計學方法
采用Cochrane系統評價軟件Revman 5.3軟件對提取的數據進行處理。各效應量使用95%的可信區間(95% confidence interval,95%CI)表示。納入研究結果間的異質性采用χ2檢驗,如P >0.1,I2<50%,則無統計學異質性,采用固定效應模型,使用加權均數差(weighted mean difference,WMD)對各指標進行分析;如P <0.1,I2>50%,則認為存在統計學異質性,采用隨機效應模型,使用標準化均數差(standardized mean difference,SMD)對各指標進行分析。以P <0.05為差異有統計學意義。
2 結果
2.1 文獻檢索及篩選結果
初檢共得到111篇文獻,剔除重復及明顯不符者,得到56篇文獻。查閱摘要后,剔除與研究內容不符者,得到13篇文獻。查找并閱讀全文,進一步對文獻進行評價,提出與納入及排除標準不符者,最終得到6篇文獻,839例患者,文獻篩選流程如圖1。
2.2 文獻特征及方法學質量評價
經檢索有6篇文獻[7-12]符合要求,并對納入的文獻根據改良Jadad量表進行評分,該量表包含隨機序列產生、隨機化隱藏、盲法、撤出與退出4個評價指標,方法恰當得2分、不清楚得1分、不恰當得0分,4項評價指標的總分1~3分為低質量研究,4~7分為高質量研究。納入研究的一般情況及Jadad評分見附表。
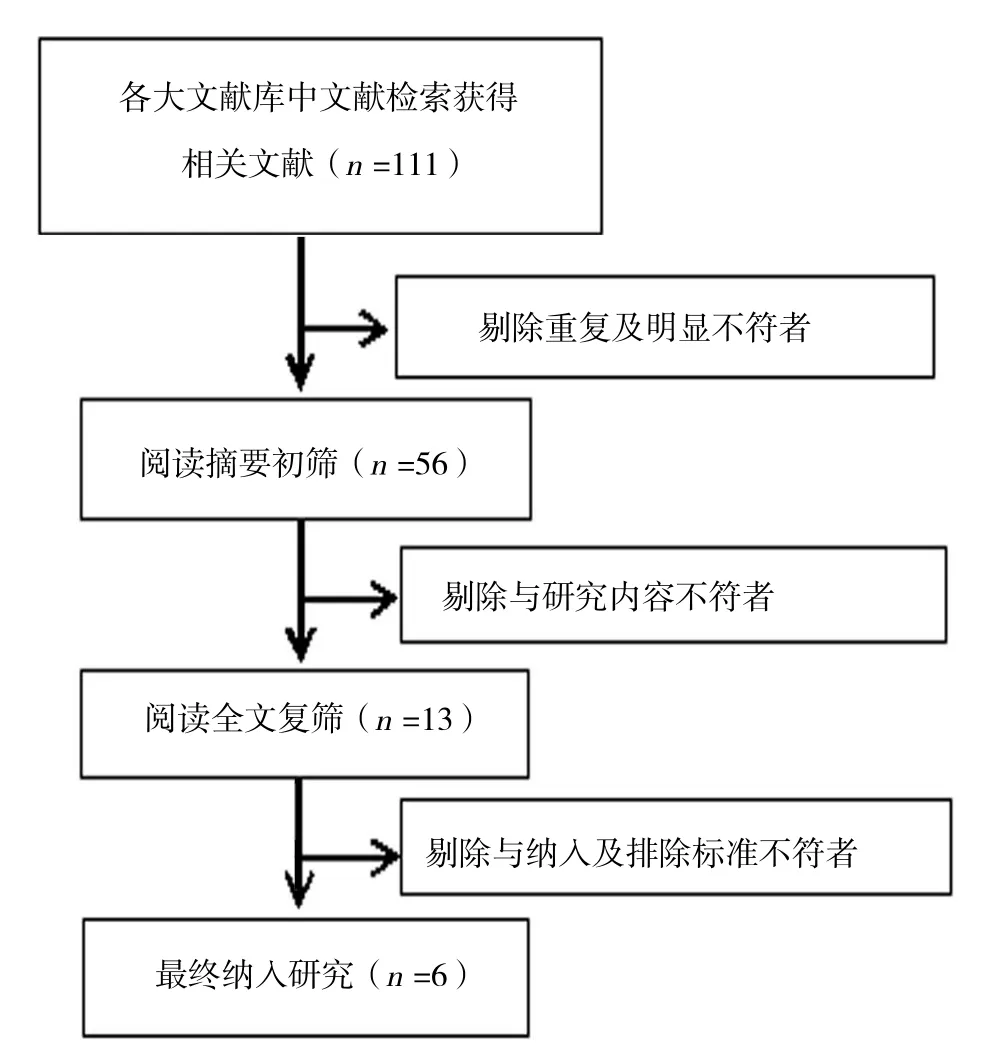
圖1 文獻篩選流程Fig.1 Flowchart of the study selection process
2.3 Meta分析結果
2.3.1 住院時間比較 有5篇文獻[8-12]描述了住院時間,各研究間存在異質性(P =0.000,I2=98%),采用隨機效應模型合并分析。Meta分析結果顯示:兩組差異有統計學意義 [SMD=-1.95,95%CI(-3.42,-0.48),P =0.009],980nm激光組住院時間比TURP組平均縮短1.95 d。見圖2。
2.3.2 手術時間比較 有6篇文獻[7-12]描述了手術時間,各研究間存在異質性(P =0.000,I2=95%),采用隨機效應模型合并分析。Meta分析結果顯示:兩組差異無統計學意義[SMD=0.11,95%CI(-0.52,0.74),P =0.730]。見圖 3。
2.3.3 留置導尿管時間 有6篇文獻[7-12]描述了留置導尿管時間,各研究間存在異質性(P =0.000,I2=98%),采用隨機效應模型合并分析。Meta分析結果顯示:兩組差異有統計學意義[SMD=-2.64,95%CI(-3.92,-1.36),P =0.000],980 nm激光組膀胱沖洗時間比TURP組平均縮短2.64 h。見圖4。
2.3.4 術后IPSS評分 有6篇文獻[7-12]描述了術后IPSS評分,各研究之間無異質性(P =0.140,I2=39%),故采用固定效應模型。Meta分析結果顯示:兩組差異無統計學意義[WMD=0.12,95%CI(-0.27,0.51),P =0.550]。見圖 5。
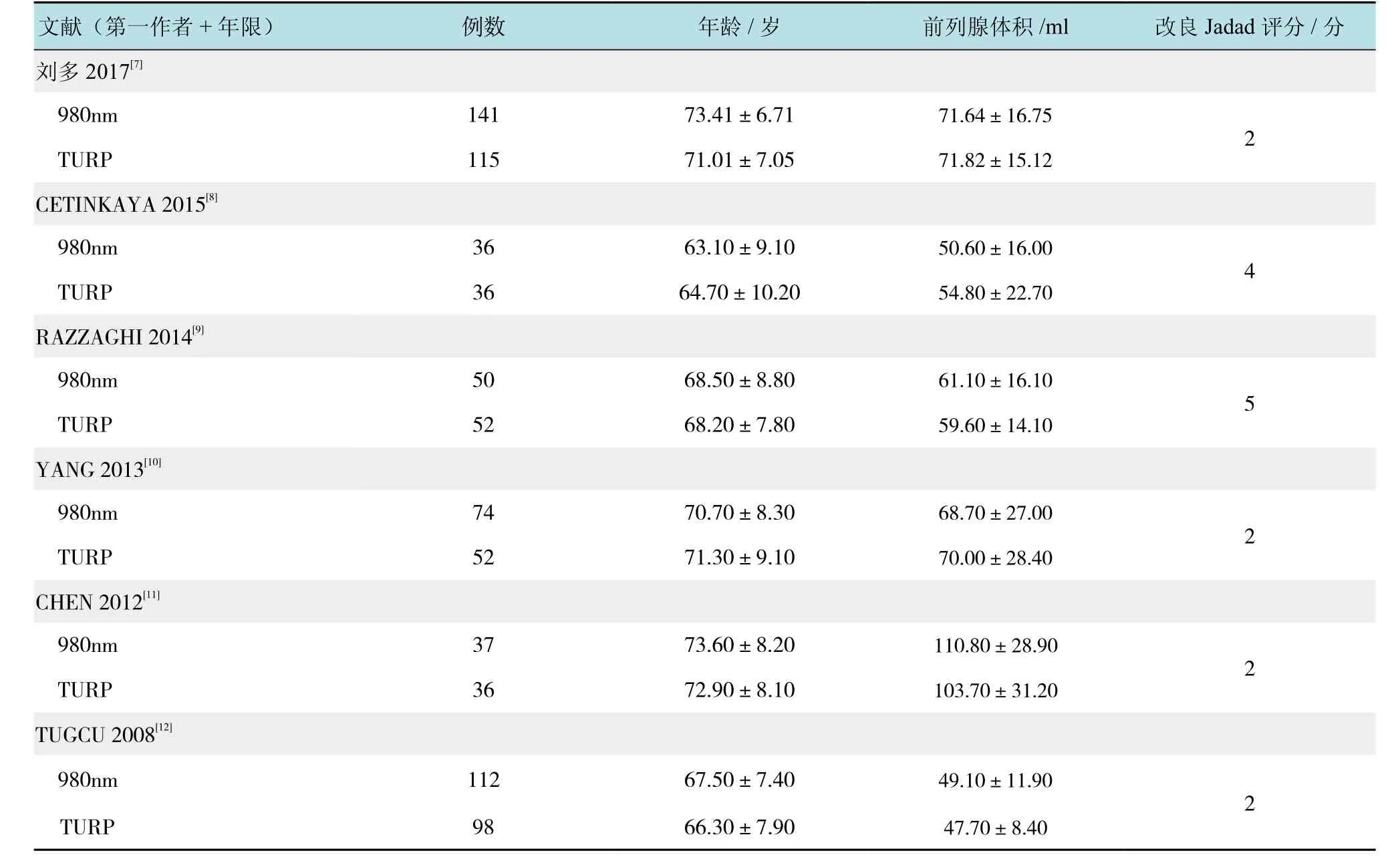
附表 納入研究的一般信息及質量評分Attached table Summary of the baseline data and Jadad score from included studies
2.3.5 術后 QOL 評分 有 3 篇文獻[8,11,12]描述了術后QOL評分,各研究間存在異質性(P =0.002,I2=84%),采用隨機效應模型合并分析。Meta分析結果顯示:兩組差異無統計學意義[SMD=0.00,95%CI(-0.57,0.57),P =0.990]。見圖 6。
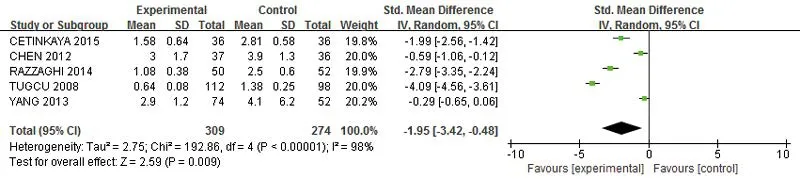
圖2 激光組和TURP組患者住院時間比較的森林圖Fig.2 Forest plot of the comparison of outcome data of hospital stays between 980 nm diode laser group and TURP group

圖3 激光組和TURP組患者手術時間比較的森林圖Fig.3 Forest plot of the comparison of outcome data of operative time between 980 nm diode laser group and TURP group
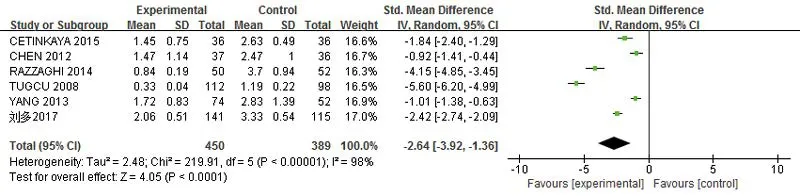
圖4 激光組和TURP組患者留置導尿管時間比較的森林圖Fig.4 Forest plot of the comparison of outcome data of catheterization time between 980nm diode laser group and TURP group
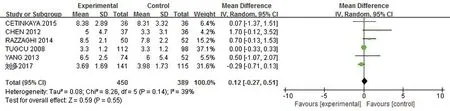
圖5 激光組和TURP組患者術后IPSS比較的森林圖Fig.5 Forest plot of the comparison of outcome data of IPSS between 980nm diode laser group and TURP group
2.3.6 術后Qmax有6篇文獻[7-12]描述了術后Qmax,各研究間存在異質性(P =0.000,I2=80%),采用隨機效應模型合并分析。Meta分析結果顯示:兩組差異無統計學意義[SMD=0.06,95%CI(-0.26,0.37),P =0.720]。見圖 7。
2.4 敏感性分析
依據Cochrane手冊,Meta分析的研究個數在10個或以上時需要做漏斗圖,本研究的納入文獻相對較少,因而未做漏斗圖。對本研究進行敏感性分析,分別使用固定效應模型和隨機效應模型計算各項指標,發現結果一致;將每個研究逐一排除后的分析顯示,靈敏度和特異度未見顯著改變。

圖6 激光組和TURP組患者術后QOL比較的森林圖Fig.6 Forest plot of the comparison of outcome data of QOL between 980nm diode laser group and TURP group
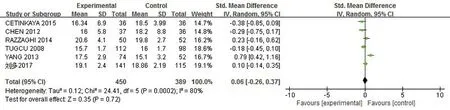
圖7 激光組和TURP組患者術后Qmax比較的森林圖Fig.7 Forest plot of the comparison of outcome data of Qmaxbetween 980nm diode laser group and TURP group
3 討論
BPH是中老年男性常見病,其發病率隨著年齡的增長而增加[1],并可能引發膀胱結石、泌尿系感染和上尿路積水等癥狀。TURP是目前手術治療的金標準[2],但它仍有不足,如術中出血較多,易并發經尿道電切綜合征等,對于高齡或合并其他嚴重疾病的患者并不合適[3]。經尿道980nm激光前列腺汽化術是治療BPH的新方法,ROCCO等[4]學者將其與包括開放手術、TURP、鈥激光前列腺剜除術(holmium laser enucleation of theprostate,HoLEP)在內多種BPH治療手段進行初步比較后發現,激光手術具有手術學習曲線短、術中術后出血少、手術視野清晰、術后恢復快和住院時間短等優點,但安全性以及中長期并發癥等方面尚需更大樣本的觀察及遠期隨訪。
本研究搜集了國內外對經尿道980nm激光汽化術與經尿道TURP治療良性BPH的療效進行比較的文獻,最終篩選出6篇文獻,并選取住院時間、手術時間、術后尿管留置時間、術后IPSS評分、術后QOL評分及術后Qmax等6個指標進行Meta分析。Meta分析顯示:980nm激光組手術時間與TURP組相當,差異無統計學意義,這說明盡管TURP的切割效率略高于980激光組,但需花費較多時間用于止血,而980nm激光由于與水和血紅蛋白有著極好的聯合吸收特性,使其在保障切割效率的同時又具有較好的止血功能,從而大大節約了手術時間[9]。另外,FAYAD等[13]研究表明由于粉碎器粉碎前列腺組織占用時間,導致HoLEP的手術時長明顯高于TURP組,這顯示980nm激光在手術效率方面的優勢。
而在住院時間和術后尿管留置時間方面980nm激光組上均短于TURP經尿道電切組。其原因在于:980nm激光組術中以生理鹽水代替TURP的甘露醇灌注液,大大降低了TURP綜合征的發生概率[10]。另外,得益于980nm激光有良好的止血效果,其明顯降低了前列腺術中術后的出血。980nm波長的半導體激光具有水與血紅蛋白的聯合吸收特性,使得其可在快速切割消融組織過程中迅速凝血,達到即刻止血的效果[7,9]。甚至有體外研究顯示,980nm波長的半導體激光在與鈥激光、綠激光等的對比中同樣有明顯的止血優勢[14]。
在術后療效方面,980nm激光組在術后IPSS評分、術后QOL評分及Qmax方面與TURP組無明顯差異,均顯示較佳的治療效果。980nm半導體激光在確保切割消融和止血效果的同時,其雙重吸收也使得前列腺的汽化平面更為平整,而且激光光纖的頭端擺動來汽化切割前列腺組織較TURP的近遠端切割的方式具有更好的操作精準性和穩定性[9]。另有研究表明,980nm波長的半導體激光治療BPH前后,前列腺特異抗原下降幅度明顯大于TURP組,提示980nm波長的半導體激光較TURP切除前列腺組織更為徹底,未來可能取得更好的療效[7]。國內還有學者利用980nm激光來治療高危高齡的BPH患者,同樣取得安全滿意的療效[15]。
本Meta分析中納入的部分指標異質性較高,主要原因是不同國家和地區、不同術者、不同時間及測量儀器間的差異等都會影響統計指標。因此,還應進行更深入的討論與研究,以使結果更加準確可靠。
綜上所述,當前證據表明經尿道980nm激光汽化術與TURP相比,在治療BPH中留置尿管時間和住院時間短,在術后恢復方面具有一定優勢,遠期效果無明顯差異。
[1]UNNIKRISHNAN R, ALMASSI N, FAREED K. Benign prostatic hyperplasia: evaluation and medical management in primary care[J]. Cleveland Clinic Journal of Medicine, 2017, 84(1): 53-64.
[2]SUZUKI Y, TOYAMA Y, NAKAYAMA S, et al. Treatment results of transurethral resection of the prostate by non-japanese boardcertified urologists for benign prostate hyperplasia: analysis by resection volume[J]. Journal of Nippon Medical School, 2017,84(2): 73-78.
[3]WU Y, DAVIDIAN M H, DESIMONE E M. Guidelines for the treatment of benign prostatic hyperplasia[J]. US Pharm, 2016,41(8): 36-40.
[4]ROCCO B, ALBO G, FERREIRA R C, et al. Recent advances in the surgical treatment of benign prostatic hyperplasia[J]. Ther Adv Urol, 2011, 3(6): 263-272.
[5]LEONARDI R, CALTABIANO R, LANZAFAME S. Histological evaluation of prostatic tissue following transurethral laser resection(TULaR) using the 980 nm diode laser[J]. Arch Ital Urol Androl,2010, 82(1): 1-4.
[6]JADAD A R, MOORE R A, CARROLL D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary[J]. Control Clin Trials, 1996. 17(1): 1-12.
[7]劉多, 范利, 劉成, 等, 經尿道半導體激光前列腺剜除術與前列腺電切術治療不同體積良性前列腺增生的臨床對比分析[J]. 中華男科學雜志, 2017, 23(3): 217-222.
[7]LIU D, FAN L, LIU C, et al. Transurethral diode laser enucleation versus transurethral electrovaporization resection of the prostate for benign prostatic hyperplasia with different prostate volumes[J].National Journal of Andrology, 2017, 23(3): 217-222. Chinese
[8]CETINKAYA M, ONEM K, RIFAIOGLU M M, et al. 980-nm diode laser vaporization versus transurethral resection of the prostate for benign prostatic hyperplasia: randomized controlled study[J]. Urology Journal, 2015, 12(5): 2355-2361.
[9]RAZZAGHI M R, MAZLOOMFARD M M, MOKHTARPOUR H, et al. Diode laser (980 nm) vaporization in comparison with transurethral resection of the prostate for benign prostatic hyperplasia: randomized clinical trial with 2-year follow-up[J].Urology, 2014, 84(3): 526-532.
[10]YANG S S, HSIEH C H, LEE Y S, et al. Diode laser (980 nm) enucleation of the prostate: a promising alternative to transurethral resection of the prostate[J]. Lasers Med Sci, 2013,28(2): 353-360.
[11]CHEN C H, CHIANG P H, LEE W C, et al. High-intensity diode laser in combination with bipolar transurethral resection of the prostate: a new strategy for the treatment of large prostates (>80 ml)[J]. Lasers Surg Med, 2012, 44(9): 699-704.
[12]TUGCU V, TASCI AI, SAHIN S, et al. Comparison of photoselective vaporization of the prostate and transurethral resection of the prostate: a prospective nonrandomized bicenter trial with 2-year follow-up[J]. J Endourol, 2008, 22(7): 1519-1525.
[13]FAYAD A S, SHEIKH M G, ZAKARIA T, et al. Holmium laser enucleation versus bipolar resection of the prostate: a prospective randomized study. Which to choose[J]. Journal of Endourology,2011, 25(8): 1347-1352.
[14]SEITZ M, ACKERMANN A, GRATZKE C, et al. Diode laser. Ex vivo studies on vaporization and coagulation characteristics[J].Urologe A, 2007, 46(9): 1242-1247.
[15]張洪博, 史慶路, 楊青松, 等. 980nm半導體激光治療高危BPH安全性分析[J]. 中華泌尿外科雜志, 2010, 31(9): 629-631.
[15]ZHANG H B, SHI Q L, YANG Q S, et al. 980 nm diode laser treatment analysis of high risk BPH[J]. Chinese Journal of Urology, 2010, 31(9): 629-631. Chinese
(吳靜 編輯)
Diode laser vaporization of prostate versus transurethral resesction of prostate in treating benign prostatic hyperplasia: a Meta-analysis*
Xiao-bo Zhang, Ming-quan Chen, Xiong Chen, Yuan-qing Dai, Guan-nan Qi,Chao Dong, Yao Bai, Xin-ji Tan, Jie Gu, Sheng Hu, Dong-jie Li
(Department of Geriatrics, Xiangya International Medical Center, Xiangya Hospital, Central South University, Changsha, Hunan 410008, China)
ObjectiveTo systematically review and evaluate the perioperative indicators and surgical curative effect of 980 nm diode laser vaporization of prostate and transurethral resesction of prostate (TURP) in treating benign prostatic hyperplasia (BPH).MethodsRetrieved published comparative studies 980 nm diode laser vaporization of prostate versus transurethral resesction of prostate in treating benign prostatic hyperplasia, and pooled the data from eligible studies. The statistical analysis was performed using Revman 5.3 software.ResultsSix trials including 839 patients were eligible to the criteria (450 in 980 nm diode laser group and 389 in TURP group). The baseline of patients characteristics were comparable in all the studies. Meta analysis showed that: the operative time was not significantly different between the 980 nm diode laser group and TURP group [SMD = 0.11, 95 ~ CI (-0.52,0.74), P > 0.05]; Compared with TURP group, 980 nm diode laser group has shorter hospital stays [SMD = -1.95,95%CI (-3.42, -0.48), P < 0.05], and shorter catheterization time [SMD = -2.64, 95%CI (-3.92, -1.36), P < 0.05].There was no significant difference between IPSS [WMD = 0.12, 95%CI (-0.27, 0.51), P > 0.05], QOL [SMD = 0.00,95%CI (-0.57, 0.57), P > 0.05] and Qmax[SMD = 0.06, 95%CI (-0.26, 0.37), P > 0.05].Conclusion980 nm diode laser vaporization of prostate is safe and effective in treating benign prostatic hyperplasia, and compared with TURP,it has advantages in shorter hospital stays and shorter catheterization time.
benign prostate hyperplasia (BPH); 980 nm diode laser vaporization of prostate; transurethral resesction of prostate (TURP)
R697.3
A
10.3969/j.issn.1007-1989.2017.07.004
1007-1989(2017)07-0016-06
2017-04-06
湖南省自然科學基金(No:14JJ7004)
李東杰,E-mail:jerry1375@126.com;Tel:13755011481
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
河北畫報(2020年10期)2020-11-26 07:20:50
科技傳播(2019年22期)2020-01-14 03:06:54
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
電子制作(2018年18期)2018-11-14 01:48:24
山東工業技術(2016年15期)2016-12-01 05:31:22
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
中國中醫藥現代遠程教育(2014年13期)2014-03-01 04:26:36
