免疫抑制治療患者乙型肝炎病毒再激活防治進展
2017-09-28 11:34:32廖成成
中國藥業 2017年18期
廖成成
(廣西醫科大學附屬腫瘤醫院,廣西 南寧 530021)
·專論·
免疫抑制治療患者乙型肝炎病毒再激活防治進展
廖成成
(廣西醫科大學附屬腫瘤醫院,廣西 南寧 530021)
目的為防治免疫抑制治療患者乙型肝炎病毒(簡稱乙肝病毒,HBV)再激活提供參考和建議。方法 通過文獻檢索,回顧性分析了免疫抑制治療患者HBV再激活的診斷、高危因素、治療藥物種類,并按照分層治療的原則系統歸納了藥物防治策略及病情監測手段等。結果與結論 免疫抑制治療患者易發生HBV再激活。抗病毒治療的啟停時機、危險分層及治療過程中乙肝病毒激活相關指標的監測是防控的關鍵。
乙型肝炎病毒;再激活;免疫抑制;防治;進展
Abstract:Ob jective To provide references and suggestions for the prevention and treatment of hepatitis B virus(HBV)reactivation in patients with immunosuppressive therapy.M ethods The literatures about the diagnosis,high risk factors and therapeutic drug types of the patients with HBV reactivation with immunosuppressive therapy were reviewed.In accordance with the principles of stratified treatment systematically summarized the drug control strategies and disease monitoring methods.Resu lts and Conclusion After immunosuppressive therapy,the patients prone to reactivation of HBV.Antiviral treatment of the start and end of the time,risk stratification and treatment of HBV activation in the monitoring of the relevant indicators is the key to prevention and control.
Key words:hepatitis B virus;reactivation;immunosuppression;prevention and treatment;progress
據統計,全球約有2.5億慢性乙型肝炎病毒攜帶者[患者乙型肝炎表面抗原(HBsAg)陽性][1]。乙型肝炎病毒(簡稱乙肝病毒,HBV)的總體流行率為3.6%[2],中國居民感染率為7.2%[3]。HBV再激活雖然可自發,但高發人群主要集中在免疫抑制治療的患者,尤其是需要長期、大量使用化學治療(簡稱化療)藥、皮質激素、單克隆抗體等免疫功能抑制藥治療的腫瘤、器官移植、風濕免疫疾病患者。如攜帶HBV的免疫抑制治療患者未進行恰當的預防和治療,輕者可導致治療中斷,影響后續治療的實施,重者可導致血清轉氨酶水平持續增高,暴發急性肝功能衰竭,甚至導致死亡[4]。為此,筆者對行免疫治療的患者HBV再激活的相關文獻進行了綜述,回顧了HBV再激活診斷、高危因素及藥物種類,并按照分層治療的原則系統地歸納了藥物防治策略及病情監測手段等。現介紹如下。
1 HBV再激活的定義及診斷
HBV再激活,是指非活動性的HBV感染患者失去針對HBV的免疫控制,在免疫重建過程中和/或免疫重建后,病毒復制突然增加。事實上,HBV再激活在國際上并無統一的診斷標準,目前使用得較多的為Perrillo R標準[5]:先前有HBV攜帶史的患者HBV DNA檢測陰性,現血清HBV DNA水平轉陽;當患者基線HBV DNA檢測陽性時,其升高超過100 U/m L;乙肝兩對半[包括乙型肝炎表面抗原及表面抗體(HBsAg,HBsAb),乙型肝炎e抗原及e抗體(HBeAg,HBeAb)和乙型肝炎核心抗體(抗 HBc)]的血清學逆轉(如先前HBsAg陰性/抗HBc陽性向HBsAg陽性轉化);排除其他感染。
2 HBV再激活的高危因素
2.1 病s毒因素
很多因素被認為與HBV再激活相關,在此主要介紹目前較肯定的HBV載量和HBsAg狀態2個因素。亦有報道稱,HBV的基因型也是其高危因素,但不同中心的研究有較大分歧[6-7],臨床對此看法存在較大爭議,尚需更多的高質量研究求證。
基線HBV DNA的高載量:高基線水平HBV DNA(如超過 104IU/m L)患者體內 HBV復制活躍,在Lau等[8]的一項涉及137例接受造血干細胞移植患者的研究中,32例高基線水平的患者(23.36%)發生肝炎,其中有13例(40.62%)發生了HBV再激活。可見,HBVDNA>105U/m L是HBV再激活最重要的危險因素。
HBsAg陽性:與HBsAg陰性者相比,HBsAg陽性患者的HBV再激活風險更高[9]。特別是HBeAg陽性并具有高基線水平的HBV DNA或出現HBsAg血清學逆轉時(HBsAg陰性/抗HBc陽性患者向HBsAg陽性轉化)。接受免疫抑制治療的HBsAg陽性腫瘤患者中,有超過14%的患者發生HBV再激活[10];相反,HBsAg陰性伴HBsAb陽性的腫瘤患者HBV再激活的風險明顯減小[11]。
2.2 疾病及治療相關因素
患者的疾病狀態、治療藥物的種類及治療方案的選擇都是影響HBV再激活的因素。當有HBV感染的血清學證據的患者接受免疫抑制相關藥物(見表1)化療和/或免疫治療及需要行器官移植、造血干細胞移植時有較高的HBV再激活風險[11-12]。因此,對以下高風險患者進行治療時應對HBV再激活的風險進行充分評估,并做好適當的預防措施。
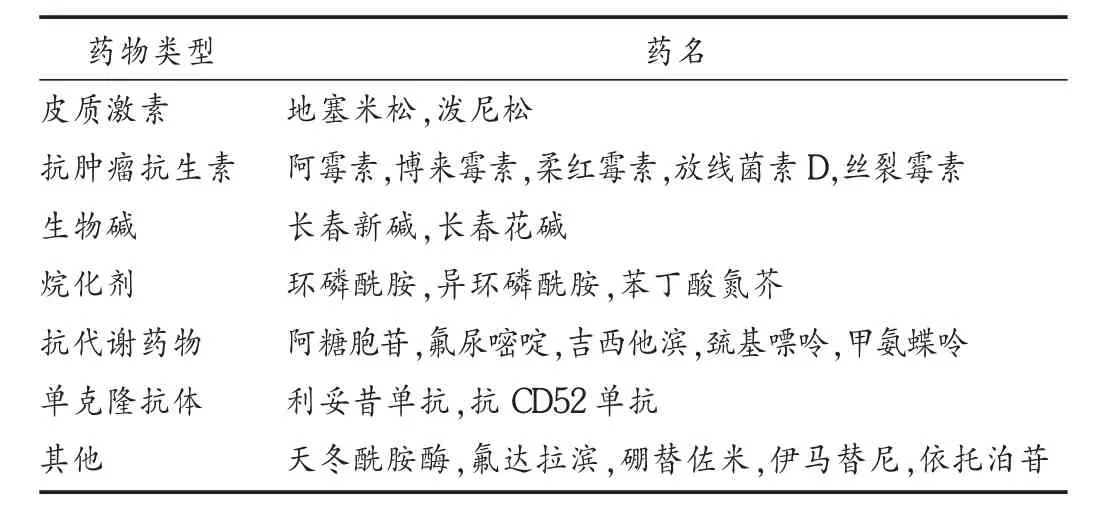
表1 已報道可引起HBV再激活的藥物
化療患者:大多數報道顯示,接受標準化療的實體瘤患者,HBV再激活的風險大于10%[13]。Kim等[14]研究發現,HBsAg陽性的乳腺癌化療患者,即便嚴密監測HBV DNA水平,HBV相關的急性肝炎發生率仍高達20%。事實上,任何化療方案都有可能導致HBV再激活,但不同腫瘤的異質性和化療方案均被認為是HBV再激活的高危因素。例如,在血液系統腫瘤中,HBV再激活的風險更大。據報道,16.3%~55.0%的淋巴瘤患者可在使用免疫化療(如利妥昔單抗+CHOP方案)后發生 HBV再激活[15]。其原因是,化療方案中同時含有利妥昔單抗、激素類藥物、細胞毒藥物,同時抑制了患者的體液免疫及細胞免疫,且利妥昔單抗半衰期較長,導致HBV復燃的概率大大增加,死亡率高達50%。
自身免疫性疾病患者:患者的HBV感染率要低于普通人群[16],這可能與干擾素(IFN)及其相關基因過表達引起自身反應的T細胞功能增強有關[17]。但已有系列病例報道證實,攜帶HBV的克羅恩病患者在接受腫瘤壞死因子(TNF)抑制劑英夫利昔單抗治療的中可能出現再激活。在80例接受英夫利昔單抗克羅恩病患者的研究中,HBsAg陽性患者死亡率高達30%[18]。此外,常見的相關藥物還有激素、甲氨蝶呤及優特克單抗(ustekinumab)等。這類患者需長期使用免疫抑制類藥物,其激活率及HBV激活相關死亡率與用藥時間及劑量強度密切相關。
移植患者:HBV再激活亦可出現在實體器官移植和造血干細胞移植的患者中。特別是HBsAg陰性的患者在行異體器官或異基因造血干細胞移植時會出現血清學逆轉,從而引起血清學復燃[19]。此外,供者的隱性感染也是一個不可忽視的因素,一項對造血干細胞移植捐贈者的隊列研究發現,在香港的隱性感染率達15.3%[20]。
3 風險分層
風險分層是精準治療的重要一步,有助于對導致患者發病的高危因素及預后進行初步判斷,為個體化治療打下基礎。美國肝病研究學會(AASLD)對免疫抑制治療中患者HBV再激活進行了風險分層[21],詳見表2。
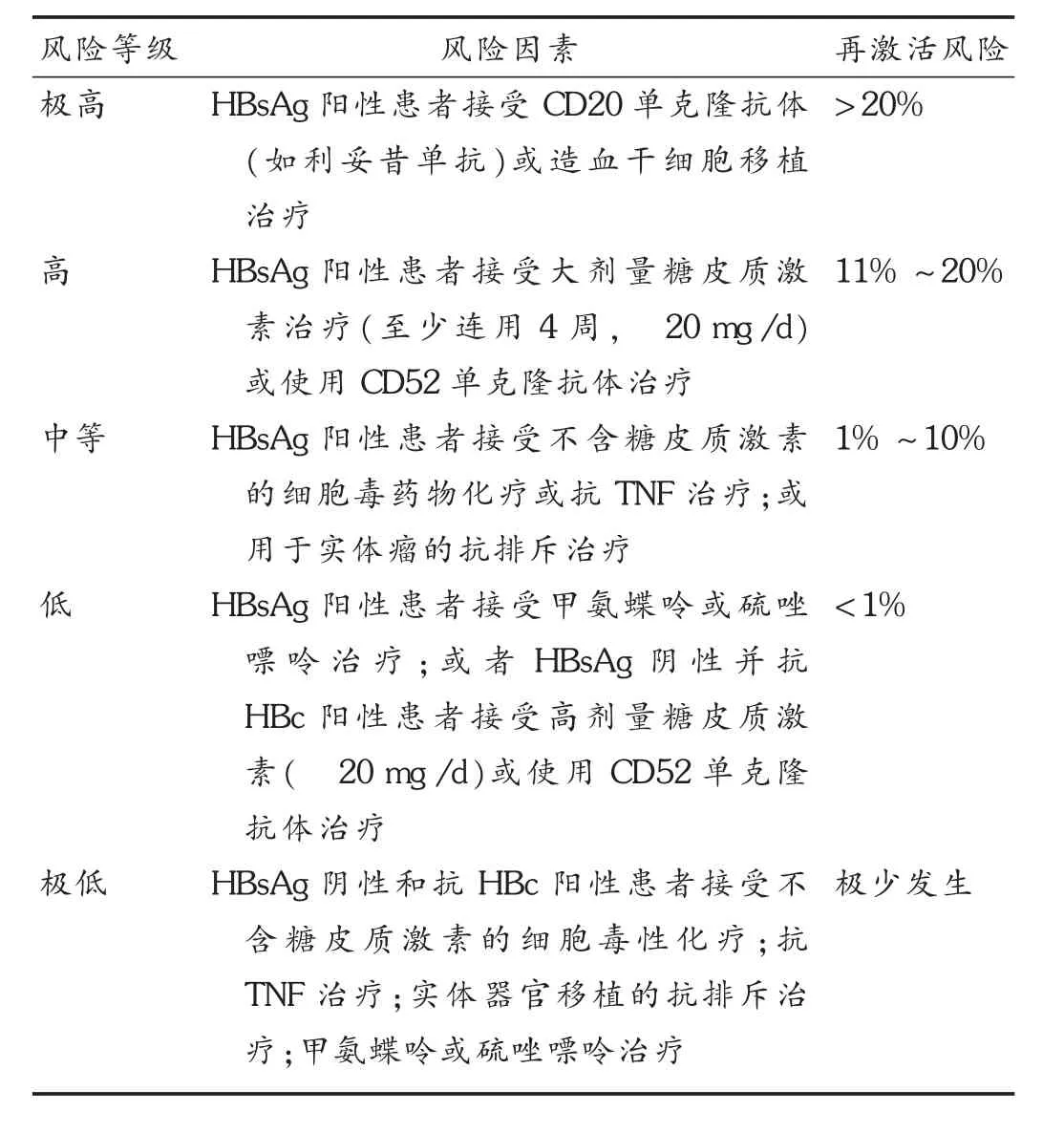
表2 HBV再激活風險分層
4 防治建議
4.1 治療時機選擇
低風險或極低風險:尚無相關研究支持HBV再激活的低風險患者需要進行預防性治療。多數指南建議進行HBV DNA監測,以便能及早發現HBV再激活并開始適當的治療[22-23]。
中等或以上風險:由表2可知,中等或以上風險的患者屬HBV再激活的高危人群。有研究表明,HBV再激活患者發生重癥肝炎或肝功能衰竭的概率高達25%~50%,一旦丙氨酸氨基轉移酶(ALT)、天門冬酸氨基轉移酶(AST)與HBVDNA載量同時升高,補救性的措施難以有效逆轉向肝功能衰竭的轉化,建議進行肝臟移植,但療效并不確切[24]。故患者滿足診斷標準應立即開始治療,而不應該根據臨床癥狀來判斷治療介入的時機。
預防性治療的啟動時機:許多研究證實,對HBV隱性感染者在免疫抑制治療之前或同時啟動的抗病毒治療可降低HBV再激活的風險。但并無數據表明在啟動免疫抑制治療前應該進行多長時間的抗病毒治療。Hwang等[25]研究達成的專家共識建議,大多數患者可在免疫抑制治療的同時啟動抗病毒治療,但對于具有高基線HBV DNA水平(>104U/mL)的患者,建議推遲免疫抑制治療,直到HBV DNA水平小于103U/m L。
4.2 治療藥物選擇
拉米夫定常用于HBV再激活的預防。隨著研究的逐漸深入,拉米夫定的耐藥率較高,甚至在HBV低載量的患者仍可發生耐藥。目前,美國肝臟病研究協會推薦使用恩替卡韋或新一代核苷酸類逆轉錄酶抑制劑(如替諾福韋酯)進行治療,先前對拉米夫定耐藥的患者可優選替諾福韋酯治療,但替諾福韋酯對腎功能的影響較恩替卡韋大,臨床應慎用。然而,抗病毒治療降低HBV再激活患者重癥肝炎發病率和病死率的證據并不多,多數報道僅顯示進行早期抗病毒治療可改善臨床預后[3,26]。
4.3 監測策略
危險分層為低危或極低危的患者(通常為抗HBc陽性,伴或不伴HBsAb陽性),推薦在化療和免疫抑制治療中及治療后進行定期的HBV相關指標檢測。對于基線可檢測到HBV DNA的患者,需每月進行相關指標監測。對于基線檢測不到HBV DNA的患者,應每3個月監測相關指標。
4.4 治療持續時間
預防和治療的持續時間大致相同,主要取決于免疫抑制的類型、化療方案的選擇及患者的基線HBV DNA水平等。一般來說,化療結束后至少應進行6個月的抗病毒治療。如使用利妥昔單抗(CD20單克隆抗體)的患者,因考慮到B細胞功能恢復的滯后性,建議停藥后至少進行12個月的治療。此外,對于行異體器官移植、異基因造血干細胞移植等需要使用長期抗排斥藥物的患者需延長治療時間,并且在抗病毒治療結束后進行長期的隨訪及監測,確保沒有肝炎的活動。
5 結語
目前,根據現有文獻和指南,免疫抑制治療患者的HBV再激活防治已有了較清晰的思路和對策,但詳細的用藥指導、藥物的啟停時機、風險分層等仍缺乏高級別的循證醫學證據,此外,藥物的成本與收益比較高、發病后治療難度大、病死率較高都是亟待攻克的難題。
[1]Schweitzer A,Horn J,Mikolajczyk RT,et al.Estimations ofworldwide prevalence of chronic hepatitis B virus infection:a systematic review of data published between 1965 and 2013[J].Lancet(London,England),2015,386(10003):1546-1555.
[2]Zhang Q,QiW,Wang X,et al.Epidemiology of Hepatitis B and Hepatitis C Infections and Benefits of Programs for Hepatitis Prevention in Northeastern China:A Cross-Sectional Study[J].Clinical Infectious Diseases,2015,62(3):305-312.
[3]CuiY,Jia J.UpdateonepidemiologyofhepatitisBand C in China[J].Journal of Gastroenterology and Hepatology,2013,28(Suppl 1):7-10.
[4]Gupta S,Govindarajan S,Fong T,et al.Spontaneous reactivation in chronic hepatitis B:patterns and natural history[J].Journal of ClinicalGastroenterology,1990,12(5):562-568.
[5]Perrillo RP,Gish R,Falck-Ytter YT.American Gastroenterological Association institute technical review on prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy[J].Gastroenterology,2015,148(1):221-244.
[6]Borentain P,Colson P,Coso D,et al.Clinical and virological factors associated with hepatitis B virus reactivation in HBsAg-negative and anti-HBc antibodies-positive patients undergoing chemotherapy and/or autologous stem cell transplantation for cancer[J].Journal of Viral Hepatitis,2010,17(11):807-815.
[7]Ozasa A,Tanaka Y,Orito E,et al.Influence of genotypes and precore mutations on fulminant or chronic outcome of acute hepatitis B virus infection[J].Hepatology,2006,44(2):326-334.
[8]Lau GKK,Leung Y,Fong DYT,et al.High hepatitis B virus(HBV)DNA viral load as themost important risk factor for HBV reactivation in patients positive for HBV surface antigen undergoing autologous hematopoietic cell transplantation[J].Blood,2002,99(7):2324-2330.
[9]Dhedin N,Douvin C,Kuentz M,et al.Reverse seroconversion of hepatitis B after allogeneic bone marrow transplantation:A retrospective study of 37 patients with pretransplant anti-HBs and anti-HBc[J].Transplantation,1998,66(5):616-619.
[10]Cil T,Altintas A,Pasa S,et al.Lamivudine for the prevention of hepatitis B virus reactivation in hepatitis-B surface antigen(HBSAG) seropositive cancer patients undergoing cytotoxic chemotherapy[J].Leukemia&Lymphoma,2008,49(5):939-947.
[11]Tanaka H,Sakuma I,Hashimoto S,et al.Hepatitis B reactivation in amultiplemyeloma patientwith resolved hepatitis B infection during bortezomib therapy:case report[J].JClin Exp Hematop,2012,52(1):67-69.
[12]Kawsar HI,Shahnewaz J,Gopalakrishna KV,et al.Hepatitis B reactivation in cancer patients:role of prechemotherapy screening and antiviral prophylaxis[J].Clinical Advances in Hematology&Oncology,2012,10(6):370-378.
[13]Paul S,Saxena AP,Terrin N,etal.Hepatitis B Virus Reactivation and Prophylaxis During Solid Tumor Chemotherapy:A Systematic Review and Meta-analysis[J].Annals of Internal Medicine,2016,164(1):30-40.
[14]Kim MK,Ahn JH,Kim SB,et al.Hepatitis B reactivation during adjuvant anthracycline-based chemotherapy in patients with breast cancer:a single institution′s experience[J].The Korean Journal of Internal Medicine,2007,22(4):237-243.
[15]YeoW,Chan TC,Leung NW,et al.Hepatitis B virus reactivation in lymphoma patients with prior resolved hepatitis B undergoinganticancer therapy with or without rituximab[J].JClin Oncol,2009,27(4):605-611.
[16]伍春霞,曾愛中.系統性自身免疫性疾病370例乙型肝炎病毒 感染臨 床分析[J].現 代醫藥衛 生,2015,31(14):2161-2162.
[17]Zhao J,Qiu M,Li M,et al.Low prevalence of hepatitis B virus infection in patientswith systemic lupuserythematosus in southern China[J].Rheumatology International,2010,30(12):1565-1570.
[18]Esteve M,Saro C,Gonzálezhuix F,et al.Chronic hepatitis B reactivation following infliximab therapy in Crohn′s disease patients:need for primary prophylaxis[J].Gut,2004,53(9):1363-1365.
[19]Hammond SP,Borchelt AM,Ukomadu C,et al.Hepatitis B Virus Reactivation following Allogeneic Hematopoietic Stem Cell Transplantation[J].Biology of Blood&Marrow Transplantation Journal of the American Society for Blood&Marrow Transplantation,2009,15(9):1049-1059.
[20]HuiCK,Sun J,Au WY,etal.Occult hepatitis B virus infection in hematopoietic stem cell donors in a hepatitis B virus endemic area[J].Journal of Hepatology,2005,42(6):813-819.
[21]Di Bisceglie AM,Lok AS,Martin P,et al.Recent US Food and Drug Administration warnings on hepatitis B reactivation with immune-suppressing and anticancer drugs:just the tip of the iceberg?[J].Hepatology,2015,61(2):703-711.
[22]王貴強,王福生,成 軍,等.慢性乙型肝炎防治指南(2015年更新版)[J].臨床肝膽病雜志,2015,31(12):1941-1960.
[23]Sarin SK,KumarM,Lau GK,etal.Asian-Pacific clinicalpractice guidelines on themanagement of hepatitis B:a 2015 update[J].Hepatology International,2016,10(1):1-98.
[24]Shih CA,Chen WC,Yu HC,et al.Risk of Severe Acute Exacerbation of Chronic HBV Infection Cancer PatientsWho Underwent Chemotherapy and Did Not Receive Anti-Viral Prophylaxis[J].PLoSOne,2015,10(8):e0132426.
[25]Hwang JP,Lok AS.Management of patientswith hepatitis B who require immunosuppressive therapy[J].Nature Reviews Gastroenterology&Hepatology,2014,11(4):209-219.
[26]Picardi M,Selleri C,De RG,et al.Lamivudine treatment for chronic replicative hepatitis B virus infection after allogeneic bone marrow transplantation[J].Bone Marrow Transplantation,1998,21(12):1267-1269.
Progress of Prevention and Treatment of Hepatitis B Virus Reactivation in Patients w ith Imm unosuppressive Therapy
Liao Chengcheng
(Affiliated Tumor Hospital of Guangxi Medical University,Nanning,Guangxi,China 530021)
R969.4;R979.5;R512.6+2
A
1006-4931(2017)18-0001-04
10.3969/j.issn.1006-4931.2017.18.001
2017-05-09;
2017-06-06)
廖成成,碩士研究生,主治醫師,研究方向為惡性腫瘤化療,(電話)0771-5390813(電子信箱)mylcc@qq.com。