頻域光學相干斷層掃描觀察早期小切口白內(nèi)障摘除聯(lián)合人工晶體植入術(shù)后黃斑區(qū)的形態(tài)變化
2017-12-11 07:38:26賈紹友丁明紅趙金亮
中國實用醫(yī)藥 2017年34期
賈紹友 丁明紅 趙金亮
【摘要】 目的 應用頻域光學相干斷層掃描(SD-OCT)觀察小切口白內(nèi)障摘除聯(lián)合人工晶體植入術(shù)后早期黃斑中心區(qū)的形態(tài)變化, 探討該術(shù)式對黃斑區(qū)的安全性。方法 選取160例(160眼)接受小切口白內(nèi)障摘除聯(lián)合人工晶體植入術(shù)患者作為病例組, 另選取29例健康志愿者作為正常對照組。對兩組受檢者的雙眼采用SD-OCT行黃斑中心凹視網(wǎng)膜厚度及黃斑區(qū)容積的檢測并進行比較。結(jié)果 正常對照組右眼黃斑中心凹視網(wǎng)膜厚度為(224.40±14.81)μm, 黃斑區(qū)容積為(8.62±0.40)mm3;左眼黃斑中心凹視網(wǎng)膜厚度為(221.05±13.25)μm, 黃斑區(qū)容積為(8.43±0.46)mm3, 正常對照組右、左眼黃斑中心凹視網(wǎng)膜厚度及黃斑區(qū)容積比較差異無統(tǒng)計學意義(P>0.05)。病例組術(shù)后3 d及1個月右眼和左眼黃斑中心凹視網(wǎng)膜厚度、黃斑區(qū)容積比較差異無統(tǒng)計學意義(P>0.05)。病例組術(shù)后3 d及1個月右眼黃斑中心凹視網(wǎng)膜厚度、黃斑區(qū)容積與正常對照組比較差異無統(tǒng)計學意義(P>0.05), 病例組術(shù)后3 d及1個月左眼黃斑中心凹視網(wǎng)膜厚度、黃斑區(qū)容積與正常對照組比較差異無統(tǒng)計學意義(P>0.05)。結(jié)論 小切口白內(nèi)障摘除聯(lián)合人工晶體植入術(shù)對黃斑中心區(qū)的形態(tài)影響較小, 安全性較高。SD-OCT是觀察小切口白內(nèi)障摘除術(shù)后早期黃斑中心區(qū)形態(tài)變化的有效方法。
【關(guān)鍵詞】 黃斑區(qū)容積;黃斑中心凹視網(wǎng)膜厚度;白內(nèi)障手術(shù);頻域光學相干斷層掃描
DOI:10.14163/j.cnki.11-5547/r.2017.34.003
Morphological changes of macula in early small incision cataract extraction combined with intraocular lens implantation by spectral-domain optical coherence tomography JIA Shao-you, DING Ming-hong, ZHAO Jin-liang. Affiliated Hospital of Qiingdao University, Qingdao 266003, China
【Abstract】 Objective To observe the morphological changes of macula in early small incision cataract extraction combined with intraocular lens implantation by spectral-domain optical coherence tomography (SD-OCT) and discuss the safety of this operation for macular region. Methods There were 160 cases (160 eyes) receiving small incision cataract extraction combined with intraocular lens implantation as case group, and
29 healthy volunteers as normal control group. The macular foveal thickness and macular volume were measured by SD-OCT in the eyes of two groups were compared. Results Normal control group had macular foveal retinal thickness in the right eye as (224.40±14.81) μm, macular volume in the right eye as (8.62±0.40) mm3, and macular foveal retinal thickness in the left eye as (221.05±13.25) μm, macular volume in the left eye as (8.43±0.46) mm3. There was no statistically significant difference in macular foveal retinal thickness and macular volume between right eyes and left eyes (P>0.05). The case group had no statistically significant difference in macular foveal retinal thickness and macular volume between right eyes and left eyes in postoperative 3 d and 1 month (P>0.05). The case group had no statistically significant difference in macular foveal retinal thickness and macular volume in the right eyes in postoperative 3 d and 1 month, comparing with the normal control group (P>0.05). The case group had no statistically significant difference in macular foveal retinal thickness and macular volume in the left eyes in postoperative 3 d and 1 month, comparing with the normal control group (P>0.05). Conclusion Combination of small incision cataract extraction and intraocular lens implantation has little influence on the shape of morphology of the central region of macula, and has higher safety. SD-OCT is an effective method to observe the morphological changes of central macular in early stage after small incision cataract extraction.endprint
【Key words】 Macular volume; Macular foveal retinal thickness; Cataract surgery; Spectral-domain optical coherence tomography
隨著白內(nèi)障手術(shù)的進步和手術(shù)設備、材料的不斷完善, 手術(shù)并發(fā)癥明顯減少, 手術(shù)效果顯著提高, 多數(shù)患者迅速恢復近乎正常的視力。為觀察小切口白內(nèi)障摘除術(shù)后早期黃斑中心區(qū)光學相干斷層掃描(OCT)的形態(tài)變化及小切口白內(nèi)障摘除術(shù)對黃斑區(qū)的安全性, 本文對小切口白內(nèi)障摘除聯(lián)合人工晶體植入術(shù)患者進行黃斑中心區(qū)頻域光學相干斷層掃描(spectral-domain optical coherence tomography, SD-OCT)檢查, 現(xiàn)分析報告如下。
1 資料與方法
1. 1 一般資料 選取2016年1~6月在本院接受小切口白內(nèi)障摘除聯(lián)合人工晶體植入手術(shù)、術(shù)中無并發(fā)癥并資料完整的160例(160眼)患者作為病例組, 其中男83例, 女77例, 年齡最大92歲, 最小55歲, 平均年齡(71.43±7.51)歲;術(shù)眼:右眼者82例, 左眼者78例。所有患者既往無眼部疾病, 無眼部手術(shù)史, 無糖尿病、高血壓、高血脂等全身疾病史。另選取29例健康志愿者作為正常對照組, 其中男16例, 女13例,
年齡50~80歲, 平均年齡(67.54±5.70)歲;裸眼視力均≥0.8;
所有志愿者均無眼部疾病。兩組年齡、性別等一般資料比較差異無統(tǒng)計學意義(P>0.05), 具有可比性。
1. 2 方法
1. 2. 1 小切口白內(nèi)障摘除聯(lián)合人工晶體植入手術(shù)方法 常規(guī)消毒鋪巾, 2%利多卡因+布比卡因3 ml球后注射, 置上直肌縫線, 做以上穹窿為基底結(jié)膜瓣, 及角膜緣后1 mm做鞏膜隧道切口至透明角膜內(nèi)1 mm, 連續(xù)環(huán)形撕囊, 水法分離, 擴大切口至5.5 mm, 挽出晶體核, 吸皮質(zhì)至清, 植入人工晶狀體, 切口自行關(guān)閉, 術(shù)后給予慶大霉素 8萬單位和地塞米松5 mg沖洗結(jié)膜囊, 包扎術(shù)眼。
1. 2. 2 SD-OCT檢測方法 使用德國Heidelberg公司Spectralis OCT儀, 對兩組受檢者的雙眼行掃描檢查。受檢者檢查時不散瞳。掃描時指示被檢者注視鏡頭內(nèi)的固視點, 對被檢眼以長度為8.8 mm的掃描線段對后極部黃斑中心凹0°和90°方
位進行掃描, 每張OCT像均由100張圖片疊加而成, 測量中心凹視網(wǎng)膜厚度值。每只眼分別獲得2個高質(zhì)量的0°和
90°方位黃斑中心凹掃描圖像。讀取所有眼0°和90°方位黃斑中心凹視網(wǎng)膜厚度, 取兩者平均值作為最終數(shù)據(jù)。數(shù)據(jù)由OCT自帶測量軟件測出。行黃斑區(qū)黃斑中心凹6.0 mm2區(qū)容積掃描, 掃描面積8.8 mm×8.8 mm, 掃描模式512×496。每張OCT像疊加16張圖片。中心凹6.0 mm2區(qū)容積數(shù)據(jù)由OCT自帶測量軟件測出。
1. 3 觀察指標 觀察兩組右眼和左眼的黃斑中心凹視網(wǎng)膜厚度、黃斑區(qū)容積, 并進行比較。
1. 4 統(tǒng)計學方法 采用SPSS22.0統(tǒng)計學軟件進行數(shù)據(jù)統(tǒng)計分析。計量資料以均數(shù)±標準差( x-±s)表示, 采用t檢驗;計數(shù)資料以率(%)表示, 采用χ2檢驗。P<0.05表示差異具有統(tǒng)計學意義。
2 結(jié)果
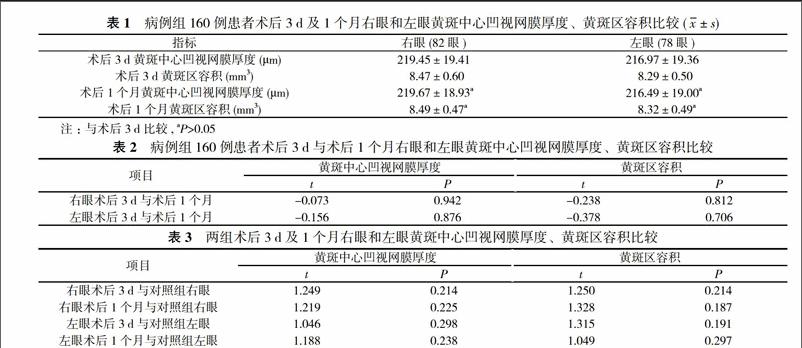
正常對照組右眼黃斑中心凹視網(wǎng)膜厚度為(224.40±
14.81)μm, 黃斑區(qū)容積為(8.62±0.40)mm3;左眼黃斑中心凹視網(wǎng)膜厚度為(221.05±13.25)μm, 黃斑區(qū)容積為(8.43±0.46)mm3, 正常對照組右眼和左眼黃斑中心凹視網(wǎng)膜厚度及黃斑區(qū)容積比較差異無統(tǒng)計學意義(P>0.05)。病例組術(shù)后3 d及1個月右眼和左眼黃斑中心凹視網(wǎng)膜厚度、黃斑區(qū)容積比較差異無統(tǒng)計學意義(P>0.05)。見表1, 表2。病例組術(shù)后3 d及1個月右眼黃斑中心凹視網(wǎng)膜厚度、黃斑區(qū)容積與正常對照組比較差異無統(tǒng)計學意義(t=1.249、1.219, 1.250、1.328, P>0.05), 病例組術(shù)后3 d及1個月左眼黃斑中心凹視網(wǎng)膜厚度、黃斑區(qū)容積與正常對照組比較差異無統(tǒng)計學意義(t=1.046、1.188, 1.315、1.049, P>0.05)。見表1, 表3。
3 討論
SD-OCT技術(shù)是一種具有高分辨率、非接觸性和無創(chuàng)傷性的組織斷層成像方法, 不僅可以從三維角度觀察黃斑區(qū)組織的細微結(jié)構(gòu)變化, 并且可定量測量黃斑中心凹視網(wǎng)膜的厚度, 定性描述黃斑區(qū)視網(wǎng)膜各層組織結(jié)構(gòu)變化, 它有利于對黃斑區(qū)病變病情進行客觀評價[1]。
黃斑水腫是白內(nèi)障摘除術(shù)后影響視力恢復的常見原因[2]。患者視功能的異常與黃斑中心凹視網(wǎng)膜厚度的改變有關(guān)[3]。白內(nèi)障摘除術(shù)中血-視網(wǎng)膜屏障的破壞與術(shù)后視網(wǎng)膜黃斑區(qū)的異常有密切相關(guān), 其發(fā)病機制尚無定論, 目前主要認為白內(nèi)障摘除術(shù)對于正常患者的血-視網(wǎng)膜屏障功能均有一定的破壞作用, 而造成視網(wǎng)膜厚度增加[4-8]。另外小切口白內(nèi)障摘除術(shù)中血-房水屏障破壞, 其炎性物質(zhì)如前列腺素、p物質(zhì)血清素、內(nèi)毒素、緩激肽、白血病素等在白內(nèi)障手術(shù)的刺激下釋放入房水, 引起黃斑部毛細血管的通透性增加以及視網(wǎng)膜色素上皮細胞排水功能的減退, 從而破壞了血-視網(wǎng)膜屏障, 可導致黃斑部視網(wǎng)膜厚度增加[9-12]。作者基于探究上述的觀點, 對160例(160眼)單純老年性白內(nèi)障患者小切口摘除聯(lián)合人工晶體植入術(shù)術(shù)后3 d及1個月的黃斑中心凹視網(wǎng)膜厚度進行了測量, 發(fā)現(xiàn)術(shù)眼術(shù)后平均黃斑中心凹視網(wǎng)膜厚度及黃斑區(qū)容積值較正常同齡人群組比較, 差異無統(tǒng)計學意義(P>0.05)。因此, 無任何并發(fā)癥的小切口白內(nèi)障摘除聯(lián)合人工晶體植入術(shù)術(shù)后短期內(nèi)對視網(wǎng)膜黃斑區(qū)無明顯影響。endprint
綜上所述, 黃斑中心凹視網(wǎng)膜厚度的測量可以反映視網(wǎng)膜局部斷層情況, 黃斑區(qū)容積測量可以反映黃斑區(qū)域的形態(tài)特征。SD-OCT能夠直觀、清晰顯示小切口白內(nèi)障摘除聯(lián)合人工晶體植入術(shù)術(shù)后早期黃斑中心凹視網(wǎng)膜厚度及黃斑區(qū)容積的形態(tài)變化, 提示小切口白內(nèi)障摘除術(shù)對黃斑區(qū)的影響較小。小切口白內(nèi)障摘除術(shù)仍是基層醫(yī)院恢復白內(nèi)障患者視功能安全、有效的手術(shù)方式。
參考文獻
[1] Biro Z, Balla Z, Kovacs B. Change of foveal and perifoveal thickness measured by OCT after phacoemulsification and IOL implantation. Eye, 2008, 22(1):8.
[2] Takamura Y, Kubo E, Akagi Y. Analysis of the effect of intravitreal bevacizumab injection on diabetic macular edema after cataract surgery. Ophthalmology, 2009, 116(6):1151-1157.
[3] Leung CK, Cheung CY, Weinreb RN, et al. Comparison of macular thickness measurements between time domain and spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci, 2008, 49(11):4893-4897.
[4] Ashwin PT, Shah S, Wolfsohn JS. Advances in cataract surgery. Clin Exp Otom , 2009, 92(4):333-342.
[5] Ghosh S, Roy I, Biswas PN, et al. Prospective randomized comparative study of macular thickness following phacoemulsification and manual small incision cataract surgery. Acta Ophthalmol, 2010, 88(4):102-106.
[6] 謝娟, 王瑞妹, 張素華, 等. 老年性白內(nèi)障術(shù)后黃斑病變的光相干斷層掃描觀察. 國際眼科雜志, 2005, 5(2):268-269.
[7] 李鵬, 安潔, 李昆, 等. 小切口白內(nèi)障囊外摘除術(shù)后黃斑區(qū)光學相干斷層掃描觀察. 西北國防醫(yī)學雜志, 2016(4):243-246.
[8] 陳志強, 謝平, 劉新亞, 等. 頻域光學相干斷層掃描對自閉式小切口白內(nèi)障摘除術(shù)后黃斑厚度的測量研究. 實用老年醫(yī)學, 2016(8):641-643.
[9] 周正申, 孫靜芬. 白內(nèi)障超聲乳化術(shù)后黃斑區(qū)光學相干斷層掃描觀察. 眼科新進展, 2013, 33(2):184-186.
[10] 龐燕華, 趙桂玲, 朱敏怡, 等. 應用頻域光學相干斷層掃描比較超聲乳化白內(nèi)障吸除術(shù)及小切口白內(nèi)障摘除術(shù)術(shù)后黃斑厚度. 齊齊哈爾醫(yī)學院學報, 2013, 34(21):3175-3177.
[11] 孔凡宏, 王艷玲, 吳勝衛(wèi), 等. 白內(nèi)障術(shù)后黃斑區(qū)光學相干斷層掃描動態(tài)觀察. 國際眼科雜志, 2014, 14(6):1023-1025.
[12] 尹江波, 劉寶海, 陳軍, 等. 超聲乳化白內(nèi)障摘除及小切口白內(nèi)障囊外摘除術(shù)后黃斑囊樣水腫的臨床研究. 山東醫(yī)學高等專科學校學報, 2016, 38(5):395-398.
[收稿日期:2017-08-14]endprint