小血管病性認知障礙與大動脈粥樣硬化性認知障礙危險因素差異的研究
2019-01-20 02:40:36安曉雷李傳玲郭靖歐春影李曉賓許可
中國醫學創新 2019年27期
安曉雷 李傳玲 郭靖 歐春影 李曉賓 許可


【摘要】 目的:探討小血管病性認知障礙(vascular cognitive impairment due to small vessel disease,VCI-SVD)與大動脈粥樣硬化性認知障礙(vascular cognitive impairment due to large artery atherosclerosis,VCI-LAA)的危險因素差異及臨床意義。方法:回顧分析110例VCI-SVD患者與102例VCI-LAA患者的人口學資料及血管危險因素,分別與100例健康體檢者比較,采用多因素logistic回歸分析,得到VCI-SVD與VCI-LAA的獨立危險因素,并比較其不同。結果:VCI-SVD組的高hs-CRP血癥、高Hcy血癥、糖尿病、高血壓、吸煙及飲酒比例均高于健康對照組,差異均有統計學意義(P<0.05)。VCI-LAA
組高血壓、腦卒中史、房顫、吸煙及飲酒比例均高于健康對照組,差異均有統計學意義(P<0.05)。logistic回歸分析顯示,糖尿病、高hs-CRP血癥、高Hcy血癥、高血壓、吸煙、飲酒是VCI-SVD特有的獨立危險因素(P<0.05);房顫、腦卒中史、高血壓、吸煙、飲酒是VCI-LAA特有的獨立危險因素(P<0.05)。結論:VCI-SVD與VCI-LAA的危險因素存在差異,針對兩種類型的認知障礙的危險因素進行有針對性的干預,能延緩或減少血管性認知障礙的出現。
【關鍵詞】 小血管病性認知障礙; 大動脈粥樣硬化性認知障礙; 危險因素
Study on the Difference of Risk Factors between Small Vascular Cognitive Impairment and Large Atherosclerotic Cognitive Impairment/AN Xiaolei,LI Chuanling,GUO Jing,et al.//Medical Innovation of China,2019,16(27):00-004
【Abstract】 Objective:To investigate the differences of risk factors and clinical significance between the VCI-SVD and VCI-LAA.Method:The demographic data and vascular risk factors of 110 patients with VCI-SVD and 102 patients with VCI-LAA were retrospectively analyzed and compared with 100 healthy people.Independent risk factors of VCI-SVD and VCI-LAA were obtained by multivariate logistic regression analysis,and their differences were compared.Result:The proportion of high hs-CRP,high Hcy,diabetes,hypertension,smoking and drinking in the VCI-SVD group were higher than those in the healthy control group,the differences were statistically significant(P<0.05).The proportion of hypertension,stroke history,atrial fibrillation,smoking and drinking in the VCI-LAA group were higher than those in the healthy control group,with statistically significant differences(P<0.05).Logistic regression analysis showed that diabetes,high hs-CRP,high Hcy,hypertension,smoking and drinking were independent risk factors specific to VCI-SVD(P<0.05).Atrial fibrillation,stroke history,hypertension,smoking and alcohol consumption were independent risk factors specific to VCI-LAA(P<0.05).Conclusion:The risk factors of VCI-SVD and VCI-LAA are different,targeted interventions for the risk factors of the two types of cognitive impairment can delay or reduce the occurrence of vascular cognitive impairment.
【Key words】 Vascular cognitive impairment due to small vessel disease; Vascular cognitive impairment due to large artery atherosclerosis; Risk factors
First-authors address:Xuzhou Central Hospital,Xuzhou 221009,China
doi:10.3969/j.issn.1674-4985.2019.27.001
隨著腦血管病患者不斷增多,血管性認知障礙(vascular cognitive impairment,VCI)患病率呈逐年遞增趨勢。VCI是指由血管因素導致從輕度認知障礙到癡呆的一類綜合征[1]。文獻[2]研究發現,大動脈粥樣硬化(large artery atherosclerosis,LAA)和小血管病(small vessel disease,SVD)是導致VCI的兩大最重要原因。目前對于VCI危險因素的研究大都集中在大動脈粥樣硬化性認知障礙(vascular cognitive impairment due to large artery atherosclerosis,VCI-LAA),而有關小血管病性認知障礙(vascular cognitive impairment due to small vessel disease,VCI-SVD) 的危險因素研究甚少。由于病理生理上的差異,VCI-SVD的危險因素與VCI-LAA的危險因素又有所不同[3-4]。本研究旨在探討VCI-SVD與VCI-LAA危險因素的差異,為臨床上對于兩種認知障礙采取有針對性的預防措施提供參考。現將研究結果報道如下。
1 資料與方法
1.1 一般資料 選取2010年3月-2014年12月就診于徐州市中心醫院神經科門診及住院的VCI患者212例,平均年齡(68.4±7.6)歲。納入標準:存在認知障礙,蒙特利爾認知評估(Montreal cognitive assessment,MoCa)評分≥26分[5-6];所有患者均接受CT或MRI檢查。排除標準:腦出血;漢密爾頓抑郁量表<17分;抑郁癥;意識障礙;有感染性、中毒、腦外傷后、硬膜下血腫、顱內占位性病變、代謝營養障礙性疾病等致認知異常者。根據TOAST分型法分型[7],其中LAA型102例,SVD型110例。另選取同期健康對照100例。所有受試者均是自愿參加本研究,并簽署知情同意書。
1.2 方法 收集患者的人口學及臨床資料,包括年齡、教育年限、性別、煙酒嗜好、高血壓、糖尿病、血脂、房顫、Hcy、hs-CRP。所有研究對象均空腹測定Hcy、hs-CRP、血糖、血脂。
1.3 血管性危險因素的診斷標準 高血壓:收縮壓≥140 mm Hg和/或舒張壓≥90 mm Hg[8]。糖尿病:2次空腹血糖>6.1 mmol/L,或2次隨機空腹血糖>7.0 mmol/L[9]。高脂血癥:高脂血癥診斷采用1997年《血脂異常防治建議》[10],血清總膽固醇≥5.7 mmol/L,或甘油三酯≥1.71 mmol/L,或低密度脂蛋白膽固醇≥3.64 mmol/L。高Hcy血癥:血Hcy≥15 μmol/L。高hs-CRP血癥:hs-CRP>3 mg/L。
吸煙:幾乎每日吸煙,平均1支/d以上,時間>1年。飲酒:每周>13次,平均50 g/d以上,時間>1年。
1.4 觀察指標 比較兩組患者與健康體檢者的人口學資料、血管危險因素。
1.5 統計學處理 采用SPSS 15.0軟件對所得數據進行統計分析,計量資料用(x±s)表示,比較采用t檢驗;計數資料以率(%)表示,比較采用字2檢驗,多因素采用非條件logistic回歸分析。P<0.05為差異有統計學意義。
2 結果
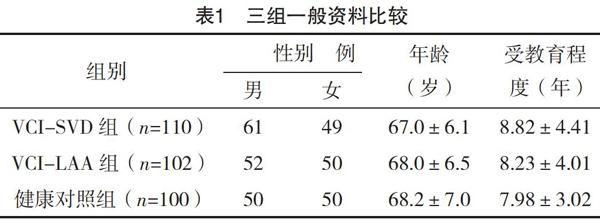
2.1 VCI-SVD組、VCI-LAA組與健康對照組人口學一般資料比較 三組患者的性別、年齡、受教育程度比較,差異均無統計學意義(P>0.05),具有可比性,見表1。
2.2 VCI-SVD組與健康對照組血管性危險因素比較 VCI-SVD組的高hs-CRP血癥、高Hcy血癥、糖尿病、高血壓、吸煙及飲酒比例均高于健康對照組,差異均有統計學意義(P<0.05);兩組高脂血癥、腦卒中史、房顫情況比較,差異均無統計學意義(P>0.05)。見表2。
2.3 VCI-LAA組與健康對照組血管性危險因素比較 VCI-LAA組高血壓、腦卒中史、房顫、吸煙及飲酒比例均高于健康對照組,差異均有統計學意義(P<0.05);兩組高hs-CRP血癥、高Hcy血癥、高脂血癥、糖尿病比較,差異均無統計學意義(P>0.05)。見表3。
2.4 非條件logistic回歸分析 將單因素分析有統計學意義的指標作為自變量,VCI-SVD及VCI-LAA為因變量,用逐步引入方法分別代入logistic方程進行多因素分析。結果顯示,在校正了其他因素后,糖尿病[OR=2.08,95%CI(1.32,4.85),P<0.05]、高hs-CRP血癥[OR=2.24,95%CI(1.38,3.91),P<0.05]、高Hcy血癥[OR=2.42,95%CI(1.23,5.62),P<0.05]、高血壓[OR=2.13,95%CI(1.22,3.65),P<0.05]、吸煙[OR=3.20,95%CI(1.03,2.23),P<0.05]、飲酒[OR=2.92,95%CI(1.08,4.75),P<0.05]是VCI-SVD特有的獨立危險因素;房顫[OR=2.15,95%CI(1.89,3.34),P<0.05]、腦卒中史[OR=3.03,95%CI(1.23,3.58),P<0.05]、高血壓[OR=2.04,95%CI(1.02,4.03),P<0.05]、吸煙[OR=2.72,95%CI(1.11,3.29),P<0.05]、飲酒[OR=2.30,95%CI(1.03,4.08),P<0.05]是VCI-LAA特有的獨立危險因素。
3 討論
根據病因及臨床表現,VCI可分為兩大類:急性起病的VCI-LAA和慢性隱襲起病的VCI-SVD,兩者的臨床特征及危險因素均有明顯的區別[11]。本研究顯示,高血壓、飲酒及吸煙是VCI-LAA和VCI-SVD的獨立危險因素(P<0.05)。分析原因可能如下:VCI-SVD導致深穿支腦小動脈病變,腦小動脈位于血液循環的最末端,與神經細胞進行物質能量交換,煙酒嗜好及高血壓病患者可促進腦小動脈平滑肌細胞纖維素樣變性,管壁增厚、管腔狹窄,導致供血區白質缺血性脫髓鞘,從而影響腦組織血液灌注而導致認知障礙[12-14]。煙酒嗜好及高血壓病患者也可導致大動脈粥樣硬化加速,導致大動脈血管壁增厚、狹窄,附壁血栓形成[15],或者促進大動脈粥樣硬化性腦梗死,相應供血區腦組織缺血缺氧從而發生VCI。本研究結果發現兩種認知障礙組中高血壓患者比例仍然有差別,VCI-SVD組高血壓比例高于VCI-LAA組。分析可能的原因是大動脈粥樣硬化患者通常伴有神經功能缺損,患者對于血壓重視程度較高,而小血管病一般起病緩慢,多數患者在出現臨床癥狀前不重視血壓的調整;另一種可能的原因是腦小血管病變導致血壓代償性增高。
hs-CRP是一種具有免疫識別和免疫調節功能的蛋白,國外研究者認為其機制是通過減少一氧化氮的產生、促進小血管平滑肌細胞增生、促進單核細胞聚集、激活補體系統等多途徑造成內皮細胞損害,從而損害認知功能[16-18]。筆者也認為hs-CRP可能通過直接或間接的作用導致血管內皮的損害,造成VCI-SVD。本研究發現,VCI-SVD組的高hs-CRP血癥比例高于VCI-LAA組。除此之外進一步校正房顫、高血壓、糖尿病、高脂血癥等相關因素后發現hs-CRP水平升高是VCI-SVD的獨立危險因素(P<0.05),但并非VCI-LAA的獨立危險因素。
血糖是VCI明確的影響因素,糖尿病引起血管基底膜增厚生化代謝紊亂,最終造成認知功能損害[19-21]。本研究發現糖尿病是VCI-SVD的獨立危險因素(P<0.05),并非VCI-LAA的獨立危險因素。分析其原因一方面由于糖尿病更容易造成腦微小血管病變;另一方面可能是由于LAA患者對于血糖更加重視,對于血糖控制更為嚴格。
目前認為Hcy誘發VCI的機制:Hcy產生自由基直接損傷血管內皮細胞,改變內皮細胞的基因表達,內皮細胞釋放血管舒張因子功能障礙,血管內皮舒張功能受損[12-13,22-23],從而導致VCI-SVD。本研究證實Hcy是VCI-SVD的獨立危險因素(P<0.05),但并非VCI-LAA的獨立危險因素,這與國外學者Bertsch等[24]研究結論一致,Bertsch等[24]研究發現,VCI-LAA組的Hcy水平與健康對照組未見明顯增高,進一步表明了Hcy可能僅損害小血管深穿動脈和微動脈,造成小血管壁增厚和透明變性,并不直接損害大動脈。
臨床中發現,VCI-LAA患者通常多有卒中病史,同時有明顯的局灶體征。而VCI-SVD患者的認知障礙常緩慢進展,一般無腦卒中病史并且神經系統局灶體征較輕。有研究對小血管病患者的追蹤發現,VCI-SVD患者多無腦卒中病史,沒有明顯的神經系統定位體征[25-26],與本研究結論一致。
本研究發現房顫是VCI-LAA的獨立危險因素(P<0.05),房顫患者栓子脫落容易進入大動脈,導致血管栓塞和心輸出量減少,由此導致腦組織低灌注有可能是形成VCI-LAA的主要原因[27]。
綜上所述,房顫、腦卒中病史是VCI-LAA特有的危險因素,糖尿病、高hs-CRP血癥、高Hcy血癥是VCI-SVD特有的危險因素。高血壓、吸煙、飲酒是兩種不同類型認知障礙的共同獨立危險因素。提示VCI-SVD與VCI-LAA有不同的危險因素和發病機制,臨床工作中要針對不同的病因,針對性地對其危險因素進行干預,減少VCI患者的出現。
參考文獻
[1]趙騰,陳海龍,劉晶瑤,等.血管性癡呆與神經束蛋白155的相關性研究[J].中國醫學創新,2015,12(30):14-16.
[2] Newhouse P,Kellar K,Aisen P,et al.Nicotine treatment of mild cognitive impairment:a 6-month double-blind pilot clinical trial[J].Neurology,2012,78(2):91-101.
[3]袁招紅,李寧,謝鵬.血管性癡呆患者血清pro-BNP水平和血脂的相關性研究[J].中國醫學創新,2017,14(19):52-55.
[4]楊軼楠,劉洪雁,蘇玉萍,等.腦梗死患者認知和記憶障礙特點分析[J].實用醫學雜志,2015,11(7):1129-1131.
[5]陳赟,何志聰,范燕明,等.簡明精神狀態量表聯合蒙特利爾認知評估量表在血管性癡呆認知功能障礙中的初步應用[J].中國醫學創新,2019,16(4):77-81.
[6] Ziad S Nasreddine,高晶.蒙特利爾認知評估量表:一個檢測輕度認知功能障礙和早期癡呆的工具[J].中華神經科雜志,2012,45(2):135-137.
[7]趙麗宏,韓杰.缺血性腦卒中TOAST分型及其復發率和危險因素分析[J].中華全科醫師雜志,2009,8(4):230-233.
[8]中國高血壓防治指南修訂委員會.中國高血壓防治指南2010[J].中華心血管病雜志,2011,39(7):579-616.
[9]曹潔瑋,劉艷,安占軍,等.阿托伐他汀鈣對冠心病合并糖尿病患者脂代謝、炎癥指標及心室重構的影響[J].中國醫學創新,2017,14(5):14-17.
[10]吳偉婷,賴樹初,黃丹敏,等.GLP-1治療2型糖尿病的臨床效果及對心腦血管并發癥的影響.血脂異常防治建議[J].中國醫學創新,2018,15(17):92-95.
[11] Villeneuve S,Belleville S,Massoud F,et al.Impact of vascular risk factors and diseases on cognition in persons with mild cognitive impairment[J].Dementia and Geriatric Cognitive Disorders,2009,27(4):375-381.
[12]安曉雷,李傳玲,郭靖,等.血管性認知功能障礙的影響因素研究進展[J].中國醫師進修雜志,2012,35(21):73-75.
[13]高展,叢文東,曾佳,等.輕度認知功能障礙與無癥狀腦梗死及病灶部位的相關性研究[J].實用醫學雜志,2013,29(11):1817-1819.
[14] Kim S H,Seo S W,Go S M,et al.Pyramidal and extrapyramidal scale(PEPS):a new scale for the assessment of motor impairment in vascular cognitive impairment associated with small vessel disease[J].Clinical Neurology and Neurosurgery,2011,113(3):181-187.
[15] Birkenh?ger W H,Forette F,Seux M L,et al.Blood pressure,cognitive functions,and prevention of dementias in older patients with hypertension[J].Archives of Internal Medicine,2001,161(2):152-156.
[16] Umemura T,Kawamura T,Umegaki H,et al.Endothelial and inflammatory markers in relation to progression of ischaemic cerebral small-vessel disease and cognitive impairment:a 6-year longitudinal study in patients with type 2 diabetes mellitus[J].J Neurol Neurosurg Psychiatry,2011,82(11):1186-1194.
[17] Imamine R,Kawamura T,Umemura T,et al.Does cerebral small vessel disease predict future decline of cognitive function in elderly people with type 2 diabetes?[J].Diabetes Research and Clinical Practice,2011,94(1):91-99.
[18] Lu D,Ren S,Zhang J,et al.Vascular risk factors aggravate cognitive impairment in first-ever young ischaemic stroke patients[J].European Journal of Neurology,2016,23(5):940-947.
[19] McNay E C,Recknagel A K.Reprint of:Brain insulin signaling:A key component of cognitive processes and a potential basis for cognitive impairment in type 2 diabetes[J].Neurobiology of Learning and Memory,2011,96(4):517-528.
[20] Yin Y,Fan Y,Lin F,et al.Nutrient biomarkers and vascular risk factors in subtypes of mild cognitive impairment:A cross-sectional study[J].The Journal of Nutrition,Health & Aging,2015,19(1):39-47.
[21] Mogi M,Horiuchi M.Neurovascular coupling in cognitive impairment associated with diabetes mellitus[J].Circ J,2011,75(5):1042-1048.
[22] Mcgimpsey S J,Woodside J V,Cardwell C,et al.
Homocysteine,methylenetetrahydrofolate reductase C677T polymorphism,and risk of retinal vein occlusion:a meta-analysis[J].Ophthalmology,2009,116(9):1778-1787.
[23] Faux N G,Ellis K A,Porter L,et al.Homocysteine,vitamin B12,and folic acid levels in Alzheimers disease,mild cognitive impairment,and healthy elderly:baseline characteristics in subjects of the Australian Imaging Biomarker Lifestyle study[J].Journal of Alzheimers Disease,2011,27(4):909-922.
[24] Bertsch T,Mielke O,H?ly S,et al.Homocysteine in cerebrovascular disease:an independent risk factor for subcortical vascular encephalopathy[J].Clinical chemistry and laboratory medicine,2001,39(8):721-724.
[25] Pohjasvaara T,M?ntyl? R,Ylikoski R,et al.Clinical features of MRI-defined subcortical vascular disease[J].Alzheimer Disease & Associated Disorders,2003,17(4):236-242.
[26]高展,叢文東,曾佳,等.輕度認知功能障礙與無癥狀腦梗死及病灶部位的相關性研究[J].實用醫學雜志,2013,29(11):1817-1819.
[27] Bunch T J,Crandall B G,Weiss J P,et al.Patients treated with catheter ablation for atrial fibrillation have long-term rates of death,stroke,and dementia similar to patients without atrial fibrillation[J].Journal of Cardiovascular Electrophysiology,2011,22(8):839-845.
(收稿日期:2019-04-22) (本文編輯:張爽)
猜你喜歡
中老年保健(2022年5期)2022-08-24 02:36:04
中老年保健(2022年5期)2022-08-24 02:35:42
中老年保健(2022年1期)2022-08-17 06:14:56
西部醫學(2021年10期)2021-10-28 08:25:50
中老年保健(2021年5期)2021-08-24 07:07:20
中老年保健(2021年11期)2021-08-22 03:15:16
當代陜西(2021年12期)2021-08-05 07:45:46
基層中醫藥(2018年4期)2018-08-29 01:25:58
基層中醫藥(2018年6期)2018-08-29 01:20:14
冰雪運動(2016年4期)2016-04-16 05:54:56