等滲劑量7.5%高滲鹽水和20%甘露醇降低顱內壓的效果比較
2019-10-19 17:29:02霍生杰張文岐金道王江峰陳琛李浩董濤
中國醫藥導報 2019年26期
關鍵詞:甘露醇
霍生杰 張文岐 金道 王江峰 陳琛李 浩 董 濤

[摘要] 目的 比較等滲劑量7.5%高滲鹽水和20%甘露醇降低顱內壓(ICP)的效果。 方法 回顧性分析陜西中醫藥大學第二附屬醫院2015年1月~2018年6月收治的重型顱腦創傷致顱內高壓患者的病例資料。其中收集符合納入標準的病例共30例,根據高滲治療方法分為7.5%高滲鹽水組(15例)和20%甘露醇組(15例)。比較兩組患者治療后ICP降低降幅、起效時間、有效持續時間、ICP最低值所需時間、腦灌注壓(CPP)、平均動脈壓(MAP)、中心靜脈壓(CVP)。分析兩組患者治療前及治療后1、3 h血鈉濃度和血漿滲透壓。 結果 7.5%高滲鹽水組治療后ICP降低幅度高于20%甘露醇組,起效時間、有效持續時間均長于20%甘露醇組,ICP最低值所需時間短于20%甘露醇組,差異均有統計學意義(均P < 0.05)。7.5%高滲鹽水組治療后CPP及MAP高于20%甘露醇組,差異有統計學意義(P < 0.05);兩組治療后的CVP比較差異無統計學意義(均P > 0.05)。兩組治療前及治療后1、3 h血漿滲透壓、血鈉濃度組內比較,差異均有統計學意義(均P < 0.05);兩組治療后1、3 h的血漿滲透壓、血鈉濃度組間比較,差異均有統計學意義(均P < 0.05)。 結論 7.5%高滲鹽水降ICP效果優于20%甘露醇。
[關鍵詞] 高滲鹽水;甘露醇;顱內壓;重型顱腦創傷
[中圖分類號] R742? ? ? ? ? [文獻標識碼] A? ? ? ? ? [文章編號] 1673-7210(2019)09(b)-0141-04
Effect comparation of isosmotic dose of 7.5% hypertonic saline and 20% mannitol on intracranial pressure reduction
HUO Shengjie? ?ZHANG Wenqi? ?LIU Jindao? ?WANG Jiangfeng? ?CHEN Chen? ?LI Hao? ?DONG Tao▲
Department of Neurosurgery, the Second Affiliated Hospital of Shaanxi University of Traditional Chinese Medicine, Shaanxi Province, Xianyang? ?712000, China
[Abstract] Objective To compare the effect of isosmotic dose of 7.5% hypertonic saline and 20% mannitol on intracranial pressure (ICP) reduction. Methods The data of patients with intracranial hypertension caused by severe traumatic brain injury admitted to the Second Affiliated Hospital of Shaanxi University of Traditional Chinese Medicine from January 2015 to June 2018 were retrospectively analyzed. Among them, 30 cases met the inclusion criteria were collected and divided into 7.5% hypertonic saline group (15 cases) and 20% mannitol group (15 cases) according to hypertonic therapy. The reduction of ICP, onset time, effective duration, minimum ICP time, cerebral perfusion pressure (CPP), mean arterial pressure (MAP) and central venous pressure (CVP) were compared between two groups. Serum sodium concentration and plasma osmotic pressure were analyzed before treatment and 1 and 3 hours after treatment between two groups. Results After treatment, ICP in 7.5% hypertonic saline group decreased more than that in 20% mannitol group, the onset time and effective duration in 7.5% hypertonic saline group were longer than that in 20% mannitol group, and the minimum ICP time in 7.5% hypertonic saline group was shorter than that in 20% mannitol group, the differences were statistically significant (all P < 0.05). CPP and MAP of 7.5% hypertonic saline group after treatment were higher than those of 20% mannitol group, the differences were statistically significant (P < 0.05). There was no significant difference in CVP between two groups after treatment (P > 0.05). There were statistically significant differences in plasma osmotic pressure and sodium concentration between two groups before treatment and 1 and 3 hours after treatment (all P < 0.05). There were statistically significant differences in plasma osmotic pressure and sodium concentration between two groups 1 and 3 hours after treatment (all P < 0.05). Conclusion ICP reduction effect of 7.5% hypertonic saline is better than that of 20% mannitol.
[Key words] Hypertonic saline; Mannitol; Intracranial pressure; Severe traumatic brain injury
顱內壓(ICP)增高是顱腦創傷后最常見臨床癥狀,而ICP升高與預后直接相關[1]。根據指南[2],當ICP超過20 mmHg(1 mmHg = 0.133 kPa)時就應該給予降ICP治療。高滲鹽水與甘露醇是臨床最常用的降ICP藥物[2],然而目前對兩者的療效認識及首選推薦存在爭議。甘露醇降ICP效果被認可,起效快,但不良反應多。而高滲鹽水,被廣泛推薦應用,研究表明高滲鹽水比甘露醇的降ICP效果好[3-4],副作用少。本研究對接受等滲劑量的7.5%高滲鹽水和20%甘露醇治療患者的病例資料進行回顧性分析,比較兩者降ICP的效果,現報道如下:
1 資料與方法
1.1 一般資料
收集陜西中醫藥大學第二附屬醫院神經外科2015年1月~2018年6月收治的重型顱腦創傷致顱內高壓患者,符合標準病例共30例(男20例,女10例)。納入標準:①年齡20~70歲;②ICP > 20 mmHg持續 5 min以上;③所有患者ICP傳感器均為腦室型;④格拉斯哥昏迷評分(GCS)5~8分。排除標準:①煩躁、吸痰、翻身等顱外因素引起ICP的升高;②嚴重的復合傷、腦死亡、腦疝或休克;③嚴重水電解質及酸堿平衡紊亂難以糾正;④合并嚴重心肺功能和凝血功能障礙。7.5%高滲鹽水組男9例,女6例;年齡20~70歲,平均(38.4±8.0)歲;20%甘露醇組男11例,女4例;年齡22~67歲,平均(36.1±15.7)歲。兩組患者性別、年齡比較差異無統計學意義(P > 0.05),具有可比性。
1.2 常規治療
依照神經外科指南[5],收住神經外科重癥監護室治療,給予置入腦室型顱內壓探測儀,持續監測ICP,常規術后1周內拔除;保持腦灌注壓> 60 mmHg;給予相應的鎮靜鎮痛治療、床頭抬高30°、維持正常體溫、保持血壓平穩及血糖濃度,不使用激素;部分患者行鎖骨下深靜脈置管;多功能監測儀監測生命體征;根據病情,部分患者行開顱手術治療;加強呼吸道管理,并給予呼吸支持。通過計算,4 mL/kg的7.5 %高滲鹽水與0.5 g/kg的20%甘露醇的滲透劑量基本相等,藥物在30 min內快速滴注完成。
1.3 觀察指標
監測并記錄患者治療后ICP降低降幅、起效時間、有效持續時間及ICP最低值所需時間;記錄患者治療后腦灌流壓(CPP)、平均動脈壓(MAP)、中心靜脈壓(CVP)及治療前和治療后1、3 h的血漿滲透壓及血鈉濃度。
1.4 統計學方法
所有數據采用SPSS 19.0軟件進行分析,計量資料以均數±標準差(x±s)表示,兩組間比較采用t檢驗,兩因素重復測量資料采用重復測量資料的方差分析。以 P < 0.05為差異有統計學意義。
2 結果
2.1 兩組患者治療后ICP相關指標比較
7.5%高滲鹽水組治療后的ICP降低幅度高于20%甘露醇組,起效時間、有效持續時間均長于20%甘露醇組,ICP最低值所需時間短于20%甘露醇組,差異均有統計學意義(P < 0.05)。見表1。
表1? ?兩組患者治療后ICP相關指標比較(x±s)
注:ICP:顱內壓;1 mmHg = 0.133 kPa
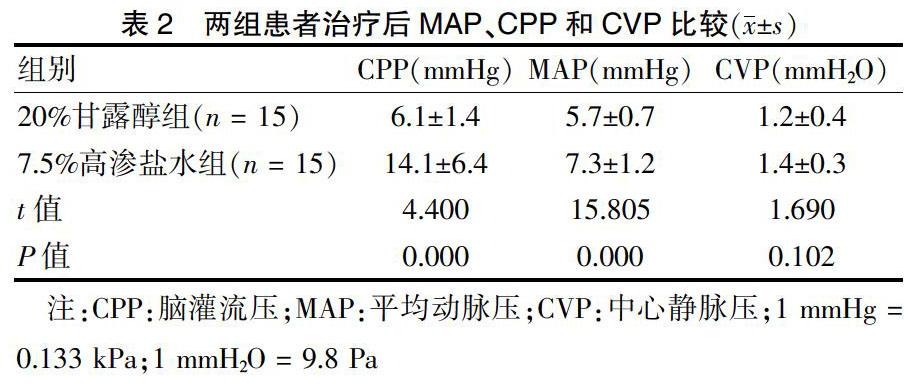
2.2 兩組患者治療后MAP、CPP和CVP比較
7.5%高滲鹽水組治療后CPP及MAP高于20%甘露醇組,差異有統計學意義(P < 0.05);兩組治療后的CVP比較差異無統計學意義(P > 0.05)。見表2。
表2? ?兩組患者治療后MAP、CPP和CVP比較(x±s)
注:CPP:腦灌流壓;MAP:平均動脈壓;CVP:中心靜脈壓;1 mmHg = 0.133 kPa;1 mmH2O = 9.8 Pa
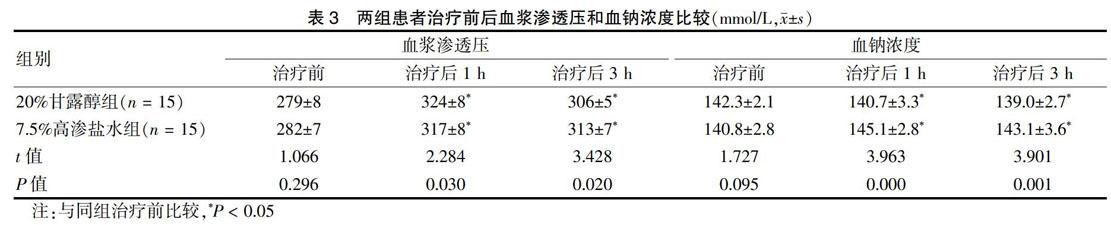
2.3 兩組患者治療前后血漿滲透壓和血鈉濃度比較
兩組治療前及治療后1、3 h的血漿滲透壓、血鈉濃度組內比較,差異均有統計學意義(P < 0.05);兩組治療后1、3 h的血漿滲透壓、血鈉濃度組間比較,差異均有統計學意義(P < 0.05)。見表3。
3 討論
顱腦創傷是現代社會嚴重影響人類健康的疾病,臨床救治中充滿巨大挑戰[6]。近年來,神經外科快速發展,推出了規范化內科及外科治療指南,接受先進的治療理念(如隆德理念)指導,致使顯著提高顱腦創傷患者的生存率,治療過程中維持ICP穩定尤為重要[7]。而高滲脫水劑是治療顱內高壓的重要方法[8-9],美國最新的《重型顱腦創傷救治指南(第四版)》[10]認為高滲藥物對顱腦創傷治療有效。
甘露醇是臨床最常用的降ICP藥物,除利尿作用外,主要通過提高血液滲透壓使腦組織的水分吸入血液,并通過腎臟排出體外,從而降低ICP[11]。甘露醇只能對正常腦組織水分有脫水作用,當血-腦積液屏障被破壞時,甘露醇可從破裂血管進入腦組織挫傷病灶區,造成病灶區腦水腫加重。對于腦缺血患者,因血管通透性增加,可導致逆向滲透。此外,甘露醇還可引起利尿相關性低血壓、急性腎功能衰竭、電解質紊亂、ICP反跳以及早期出血增加等并發癥,使用甘露醇應更加謹慎[12]。相反,高滲鹽水逐漸被國內外學者推薦應用[13],通過直接提高細胞外液鈉離子濃度、增加血漿滲透壓脫水來降低ICP,對內環境平衡的影響小,不會導致利尿性低血壓[14]。高滲鹽水不僅可以為細胞內環境提供必需的鈉離子,有利于鈉鉀泵功能正常,可保持細胞體積及維持細胞靜息電位,也可以升高CPP和增加腦組織氧合[15]。對于顱高壓危象、惡性顱高壓及腎功能不全的患者,使用高滲鹽水效果更好;尤其兒童患者,高滲鹽水被唯一推薦使用[16]。雖然高滲鹽水療效被認可,特別是用于難治性ICP升高,但缺乏最有效濃度或劑量的證據,并存在相關并發癥,如低血鉀、一過性酸中毒、高鈉血癥等。偶有引起腎功能衰竭,當在糾正低鈉血癥過快時可引起腦橋中央髓鞘溶解,臨床少見[17]。
[11]? Tang SC,Lin RJ,Shieh JS,et al. Effect of mannitol oncerebrovascular pressure reactivity in patients with intracranialhypertension [J]. J Formos Med Assoc,2015, 114(9):842-848. doi:10.1016/j.jfma.2013.09.002.
[12]? Mangat HS,Hrtl R. Hypertonic saline for the management of raised intracranial pressure after severe traumatic brain injury [J]. Ann NY Acad SCI,2015(1345):83-88.
[13]? Stewart R,Ghamande S,White H,et al. Protocol for administration of hypertonic saline in medical intensive care patients with severe stroke [J]. Chest,2016,150(4):230A.
[14]? Ali A,Tetik A,Sabanci PA,et al. Comparison of 3% hypertonic saline and 20% mannitol for reducing intracranial pressure in patients undergoing supratentorial brain tumor surgery:a randomized,double-blind clinical trial [J]. J Neurosurg Anesthesiol,2018,30(2):171-178.
[15]? Prabhakar H,Singh GP,Anand V,et al. Mannitol versushypertonic saline for brain relaxation in patients undergoing craniotomy [J]. Sao Paulo Med J,2015,133(2):166-167.
[16]? Ockswold GL,Solid CA,Paredes-Andrade E,et al. Hypertonic saline and its effect on intracranial pressure,cerebral perfusion pressure,and brain tissue oxygen [J]. Neurosurgery,2009,65(6):1035-1041.
[17]? Lazaridis C,Neyens R,Bodle J,et al. High oasmolarity saline in neurocritical care:systematic review and meta-analysis [J]. J Neurosury,2012,116(1):210-221.
[18]? 楊細平,張馨予,涂悅,等.不同濃度高滲鹽水對顱腦創傷后顱內高壓患者的療效觀察[J].天津醫藥,2017,45(8):810-814.
[19]? Kochanek PM,Carney N,Adelson PD,et al. Guidelines for the acute medical management of severe traumatic brain injury ininfants,children,and adolescents-second edition [J]. Pediatr Crit Care Med,2012,13(Suppl 1):S1-S82.
[20]? 柴磊,楊彥龍,孫紅星,等.等滲透劑量的7.5%高滲鹽水和20%甘露醇治療顱內高壓療效的對比研究[J].現代生物醫學進展,2015,15(29):5728-5731.
[21]? Ichai C,Armando G,Orban JC,et al. Sodium lactate versus mannitol in the treatment of intracranial hypertensive episodesin severe traumatic brain-injured patients [J]. Intensive Care Med,2009,35(3):471-479.
(收稿日期:2019-01-15? 本文編輯:李亞聰)
猜你喜歡
云南醫藥(2021年6期)2022-01-08 04:07:38
中國民間療法(2021年5期)2021-06-09 09:21:26
華聲文萃(2019年12期)2019-09-10 07:22:44
中西醫結合心血管病電子雜志(2017年17期)2017-11-17 15:54:41
上海農業學報(2017年4期)2017-04-10 12:40:22
中西醫結合心血管病雜志(電子版)(2017年17期)2017-01-11 06:37:25
食藥用菌(2016年6期)2016-03-01 03:24:27
中國繼續醫學教育(2015年4期)2016-01-07 07:38:11
護士進修雜志(2015年5期)2015-03-18 19:22:53
中國藥業(2014年24期)2014-05-26 09:00:09