130例急診室消化道出血患者病因及實驗室結果分析
2020-04-08 01:22:16初禎
中國現代醫生 2020年3期
初禎

[摘要] 目的 分析急診室消化道出血患者病因及實驗室檢查結果。 方法 收集2018年1月~2019年1月我院急診室收治的130例診斷為消化道出血患者的臨床資料,進行回顧性分析,采用SPSS17.0進行統計學分析。 結果 130例急性消化道出血患者中,導致上消化道出血的常見病因包括胃潰瘍(40.00%)、胃癌(37.50%)等,而導致下消化道出血的常見病因為直腸癌(52.00%)、結腸癌(20.00%)等;上消化道出血患者的血紅蛋白、總蛋白、乳酸脫氫酶明顯低于下消化道出血患者,肌酐值明顯高于下消化道出血患者,差異有統計學意義(P<0.05)。 結論 加強對急診室消化道出血患者臨床特征的認識,有助于急診室醫生盡快做出診斷及治療。
[關鍵詞] 消化道出血;內窺鏡檢查;實驗室檢查;急診室
[中圖分類號] R57? ? ? ? ? [文獻標識碼] B? ? ? ? ? [文章編號] 1673-9701(2020)03-0123-03
[Abstract] Objective To analyze the etiology and laboratory results of patients with gastrointestinal hemorrhage in emergency room. Methods The clinical data of 130 patients diagnosed with gastrointestinal hemorrhage admitted to the emergency room of our hospital from January 2018 to January 2019 were collected and retrospectively analyzed. SPSS 17.0 was used for statistical analysis. Results Among the 130 patients with acute gastrointestinal hemorrhage, the common causes of upper gastrointestinal hemorrhage included gastric ulcer(40.00%) and gastric cancer(37.50%). The common cause of lower gastrointestinal hemorrhage was rectal cancer(52.00%) and colon cancer(20.00%), etc. Hemoglobin, total protein, lactate dehydrogenase in patients with upper gastrointestinal hemorrhage were significantly lower than those in lower gastrointestinal hemorrhage, and creatinine value was significantly higher than that in lower gastrointestinal hemorrhage, and the difference was statistically significant(P<0.05). Conclusion Strengthening the understanding of the clinical features of patients with gastrointestinal hemorrhage in the emergency room can help the emergency room doctor to make diagnosis and treatment as soon as possible.
[Key words] Gastrointestinal hemorrhage; Endoscopy; Laboratory examination; Emergency roomc
急性消化道出血是全球主要的醫療急癥[1]。其中急性上消化道出血是胃腸病學中最主要的醫療急癥,主要分為非靜脈曲張性出血和靜脈曲張性出血兩類,干預措施包括輸血、內窺鏡治療、介入或手術[2]。盡管隨著幽門螺旋桿菌根治方法的進展,質子泵抑制劑及內窺鏡的及時應用使上消化道出血的發生率較前有所下降,但仍與5%~10%的死亡率相關[3]。急性下消化道出血也是急診醫學中常見的醫學問題,常見病因包括惡性腫瘤、息肉類疾病、炎癥性疾病、憩室、血管畸形及全身系統性疾病累及腸道等[4]。下消化道出血通常不如上消化道出血嚴重,出血可自發停止[5,6]。為了解急診室消化道出血患者的流行病學及臨床特征,對我院急診科130例消化道出血患者的臨床資料進行回顧性分析。促使臨床醫生對急診室消化道出血患者的流行病學及臨床特征有進一步的認識,為臨床診斷和治療提供幫助,現報道如下。
1 資料與方法
1.1 一般資料
選取2018年1月~2019年1月我院急診室收治的130例診斷為消化道出血的患者,其中上消化道出血患者80例,年齡45~83歲,平均(61.38±6.17)歲;下消化道出血患者50例,年齡46~85歲,平均(63.57±8.32)歲。納入標準:(1)年齡≥18歲;(2)以嘔血、黑便或血便為主訴者;(3)有完整病史、實驗室檢查(血細胞分析、肝腎功能、血型、凝血功能)和內窺鏡或腹部影像學檢查結果者。排除標準:(1)臨床資料記錄不完整者;(2)診斷不明確者;(3)年齡<18歲。
1.2 方法
收集符合納入標準的患者的病歷資料,記錄患者年齡、性別、首發癥狀、既往病史、生命體征、實驗室及影像學檢查結果及內窺鏡檢查結果。
1.3 統計學方法
采用SPSS17.0統計學軟件進行分析,計數資料以[n(%)]表示,采用χ2檢驗,計量資料若符合正態性分布,以均數±標準差(x±s)表示,采用t檢驗,P<0.05為差異有統計學意義。
2 結果
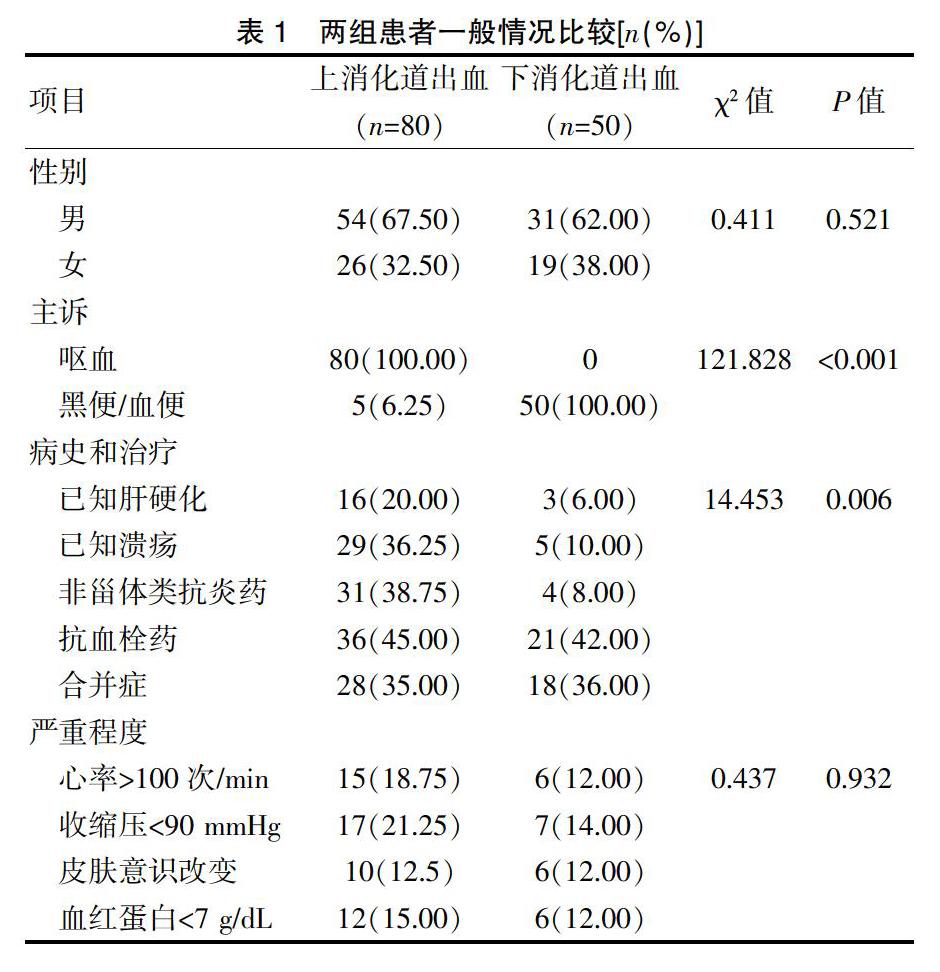
2.1 兩組患者一般情況比較
130例急性消化道出血患者中,上消化道出血患者80例,下消化道出血患者50例,見表1。
2.2? 兩組患者病因分析
130例急性消化道出血患者中,導致上消化道出血的常見病因包括胃潰瘍32例(40.00%)、胃癌30例(37.50%)等,而導致下消化道出血的常見病因為直腸癌26例(52.00%)、結直腸癌10例(20.00%)等。見表2。
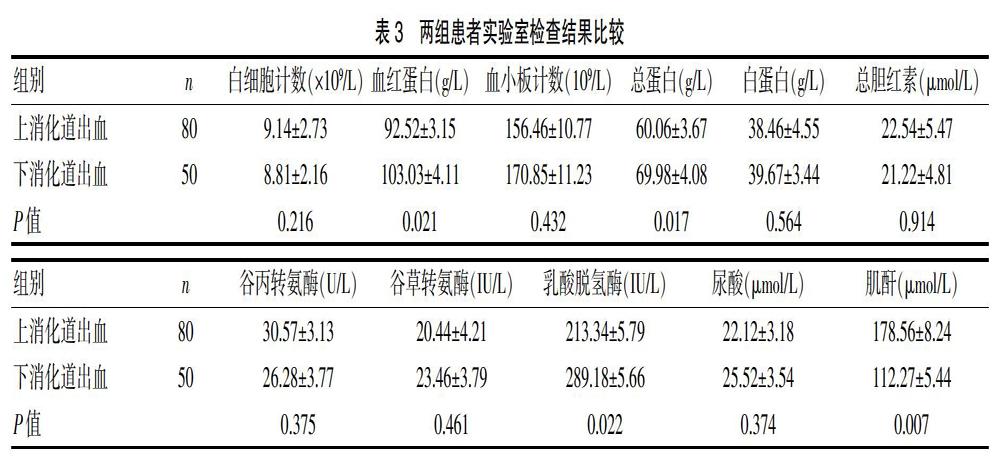
2.3 兩組患者實驗室檢查結果比較
130例急性消化道出血患者中,上消化道出血患者的血紅蛋白、總蛋白、乳酸脫氫酶明顯低于下消化道出血患者(P<0.05),肌酐值明顯高于下消化道出血患者(P<0.05),差異有統計學意義。見表3。
3 討論
急性上消化道出血是指十二指腸懸韌帶以上的消化道包括食管、胃、十二指腸、膽管及胰管等病變引起的出血。每年發病率為100/10萬~180/10萬[7],大多數患者尤其是大量出血患者首診于急診科。主要臨床表現為嘔血、黑便,也可以出現頭暈、乏力等不典型癥狀。根據病因主要分為非靜脈曲張性出血及靜脈曲張性出血,臨床上非靜脈曲張性出血占急性上消化道出血的80%~90%,其中常見病因包括胃十二指腸潰瘍、食道炎、惡性腫瘤等[8,9]。
急性下消化道出血定義為十二指腸懸韌帶遠端出血,或源自結腸或直腸的便血發作。約占所有消化道出血的20%[10]。雖然大多數急性下消化道出血患者會自發停止出血且預后良好,但在老年患者及有并發癥的患者中,發病率及死亡率會有增加[11]。典型臨床表現為便血(栗色或紅色血液通過直腸排出)突然發作。但少數情況下,也可表現為黑便(黑色,柏油樣便)[12]。
在本研究中,急性下消化道出血患者所占比例較高(50/130),且主要為結直腸癌患者,可能與本地區經濟欠發達,老年惡性腫瘤患者未能早期發現或盡早治療相關,應加強惡性腫瘤的三級預防,做到早期發現、早期診斷、早期治療。就診于急診科的消化道出血患者普遍較重,大量嘔血患者可伴有黑便,甚至血便,應注意與下消化道出血相鑒別。急診科醫生應盡快對患者進行評估及處置,尤其對伴有生命體征不平穩及皮膚、意識有改變的患者高度警惕。待患者病情穩定、出血控制后根據原發疾病轉入專科病房繼續治療或出院隨訪。
有研究表明,部分實驗室檢查結果可用于區分上消化道出血和下消化道出血[13]。上消化道出血組的血紅蛋白(P=0.023),總蛋白(P=0.0002)和乳酸脫氫酶(P=0.009)顯著低于下消化道出血組;上消化道出血組血肌酐值顯著高于下消化道出血組(P=0.0065)。Logistic回歸分析顯示,血肌酐值與上消化道出血和下消化道出血的診斷密切相關。ROC分析顯示閾值血肌酐值為21.0 mg/dL,特異性為93.0%[14]。
在本研究中,上消化道出血患者的血紅蛋白、總蛋白、乳酸脫氫酶明顯低于下消化道出血患者(P<0.05),肌酐值明顯高于下消化道出血患者(P<0.05),差異有統計學意義,與以往研究結果相符。消化道出血容易出現漏診,在臨床工作中應盡量降低漏診率[15]。實驗室檢查創傷小,費用低,方便易行,在內窺鏡檢查前行實驗室檢查不僅可以幫助臨床醫生判斷患者嚴重程度,還可以輔助鑒別上消化道出血和下消化道出血,為急診科醫生盡快做出評估及處置提供很大幫助。
本文對130例急診室消化道出血患者的臨床資料及實驗室檢查結果進行了簡單的回顧性分析,初步分析了急性消化道出血患者的病因,比較了實驗室檢查結果在上消化道出血患者和下消化道出血患者中的差異,希望對急診室醫生的診斷和治療提供一定的幫助。
[參考文獻]
[1] Stanley AJ,Laine L,Dalton HR,et al. Comparison of risk scoring systems for patients presenting with upper gastrointestinal bleeding:International multicentre prospective study[J]. BMJ,2017,356:i6432.
[2] 張明清,涂家紅,王海英,等. 急性上消化道出血的病因及相關因素分析[J]. 臨床急診雜志,2017,(9):40-43.
[3] Cremers I,Ribeiro S. Management of variceal and nonvariceal upper gastrointestinal bleeding in patients with cirrhosis[J]. Therap Adv Gastroenterol,2014,7(5):206-216.
[4] Marion Y,Lebreton G,Le Pennec V,et al. The management of lower gastrointestinal bleeding[J]. J Visc Surg,2014,151:191-201.
[5] Venkatesh PG,Njei B,Sanaka MR,et al. Risk of comorbidities and outcomes in patients with lower gastrointestinal bleeding-a nationwide study[J]. Int J Colorectal Dis,2014,29(8):953-960.
[6] Feinman M,Haut ER. Lower gastrointestinal bleeding[J]. Surg Clin North Am,2014,94:55-63.
[7] Jaorath V,Kahan BC,Stanworth SJ,et al. Prevalence,management,and outcomes of patients with coagulopathy after acute nonvaiceal upper gastrointestinal bleeding in the United Kingdom[J]. Transfusion,2013,53(5):1069-1076.
[8] Kim KB,Yoon SM,Youn SJ. Endoscopy for nonvariceal upper gastrointestinal bleeding[J]. Clin Endosc,2014,47(4):315-319.
[9] Thiebaud PC,Yordanov Y,Galimard JE,et al. Management of upper gastrointestinal bleeding in emergency departments,from bleeding symptoms to diagnosi:A prospective,multicenter,observational study[J]. Scand J Trauma Resusc Emerg Med,2017,25(1):78.
[10] Chan FKL. Lower gastrointestinal bleeding:What have we learned from the past 3 decades?[J].Clininal Gastroenterol Hepatol,2015,13(3):495-497.
[11] Oakland K,Guy R,Uberoi R,et al. Acute lower GI bleeding in the UK:Patient characteristic,interventions and outcomes in the first nationwide audit[J]. Gut,2018, 67:654-662.
[12] Sengupta N,Tapper EB,Patwardhan VR,et al. Risk factors for adverse outcomes in patients hospitalized with lower gastrointestinal bleeding[J]. Mayo Clin Proc,2015, 90(8):1021-1029.
[13] Tomizawa M,Shinozaki F,Hasegawa R,et al. Reduced hemoglobin and increased C-reactive protein are associated with upper gastrointestinal bleeding[J]. World J Gastroenterol,2014,20(5):1311-1317.
[14] Tomizawa M,Shinozaki F,Hasegawa R,et al. Laboratory test variables useful for distinguishing upper from lower gastrointestinal bleeding[J]. World J Gastroenterol,2015, 28:6246-6251.
[15] 陳濤,張艷梅,劉暢. 膠囊內鏡對不明原因消化道出血的漏診原因[J]. 中國現代醫生,2017,55(16):74-76.
(收稿日期:2019-10-22)
