不同途徑應用替羅非班對急性ST段抬高型心肌梗死患者PCI術后炎癥因子及內皮功能影響
2021-06-02 06:00:20方存明伍超胡學俊劉冰
中國醫學創新 2021年11期
關鍵詞:炎癥因子
方存明 伍超 胡學俊 劉冰
【摘要】 目的:探討不同途徑應用替羅非班對急性ST段抬高型心肌梗死患者經皮冠狀動脈介入治療(PCI)術后炎癥因子及內皮功能的影響。方法:選擇2018年1月-2019年3月本院心血管內科收治的擬行PCI術的急性ST段抬高型心肌梗死患者110例。按隨機數字表法將患者分為對照組55例和觀察組55例。對照組患者給予常規治療+替羅非班外周靜脈滴注,首次計量為10 μg/kg,再以0.15 μg/(kg·min)經微量注射泵持續靜脈泵入24 h;觀察組患者常規治療+替羅非班經冠狀動脈內注射用藥,首次用藥劑量為10 μg/kg,再以0.15 μg/(kg·min)經微量注射泵行持續靜脈注射24 h。比較兩組患者術后血清CyPA、hs-CRP、MMP-9、NO、VEGF、vWF水平及不良反應發生情況。結果:術前及術后1 d,兩組血清CyPA、hs-CRP、MMP-9、NO、VEGF、vWF比較,差異均無統計學意義(P>0.05);與術前相比,術后1 d,兩組血清CyPA、hs-CRP、MMP-9、VEGF、vWF均明顯升高,血清NO濃度均明顯下降,差異均有統計學意義(P<0.05)。術后1周,兩組血清CyPA、hs-CRP、MMP-9、VEGF、vWF均較術后1 d明顯下降,且觀察組均明顯低于對照組,差異均有統計學意義(P<0.05)。術后1周,兩組血清NO均較術后1 d升高,且觀察組高于對照組,差異均有統計學意義(P<0.05)。對照組不良反應發生率為18.2%,觀察組不良反應發生率為18.2%,兩組患者治療期間的不良反應發生率比較,差異無統計學意義(P>0.05)。結論:在常規治療的基礎上,替羅非班經冠狀動脈內注射用藥與外周靜脈用藥相比,可明顯降低急性心肌梗死患者PCI術后血清CyPA、hs-CRP、MMP-9、vWF、VEGF濃度,提高血清NO濃度,且未增加不良反應的發生。
【關鍵詞】 替羅非班 心肌梗死 炎癥因子
[Abstract] Objective: To investigate the effects of Tirofiban on inflammatory factors and endothelial function in patients with acute ST-segment elevation myocardial infarction after percutaneous coronary intervention (PCI). Method: A total of 110 patients with acute ST-segment elevation myocardial infarction who planned to undergo PCI were enrolled in the department of cardiology of our hospital from January 2018 to March 2019. According to random number table method, the patients were divided into control group 55 cases and observation group 55 cases. Control group was given conventional treatment + peripheral intravenous infusion of Tirofiban, the first dose was 10 μg/kg, and then 0.15 μg/ (kg·min) through microinjection pump for 24 h continuous intravenous infusion. Observation group was treated with routine therapy + Tirofiban intra-coronary injection, the first dose was 10 μg/kg, and then 0.15 μg/ (kg·min) through micro injection pump for continuous intravenous injection for 24 h. The levels of serum CyPA, hs-CRP, MMP-9, NO, VEGF, vWF and the incidence of adverse reactions were compared between two groups after operation. Result: Before and 1 d after surgery, there were no significant differences in serum CyPA, hs-CRP, MMP-9, NO, VEGF and VWF between the two groups (P>0.05). Compared with preoperation, 1 d after operation, serum CyPA, hs-CRP, MMP-9, VEGF and vWF were significantly increased in both groups, while serum NO concentration were significantly decreased, the differences were statistically significant (P<0.05).
1 week after operation, the serum CyPA, hs-CRP, MMP-9, VEGF, vWF in both groups were significantly decreased compared with 1 d after operation, and the observation group were significantly lower than those of the control group, the differences were statistically significant (P<0.05). 1 week after operation, serum NO in both groups were higher than those on 1 d after operation, and the observation group was higher than the control group, the differences were statistically significant (P<0.05). The incidence of adverse reactions in the control group was 18.2%, and the incidence of adverse reactions in the observation group was 18.2%, there was no statistical significance in the incidence of adverse reactions between the two groups during treatment (P>0.05). Conclusion: On the basis of conventional treatment, Tirofiban intra-coronary injection compared with peripheral intravenous administration significantly reduced serum concentrations of CyPA, hs-CRP, MMP-9, vWF and VEGF in patients with acute myocardial infarction after PCI, increased serum NO concentration, and did not increase the occurrence of adverse reactions.
[Key words] Tirofiban Myocardial infarction Inflammatory factors
First-authors address: The Peoples Hospital of Xuancheng City, Xuancheng 242000, China
doi:10.3969/j.issn.1674-4985.2021.11.016
急性ST段抬高型心肌梗死是在冠狀動脈粥樣硬化基礎下斑塊破裂,誘導血小板聚集、血栓形成,導致持續冠脈閉塞引起心肌梗死,是冠心病嚴重并發癥之一。經皮冠狀動脈介入術(PCI)能迅速開通閉塞冠脈,是恢復冠脈血流、改善心肌供血最有效的方法[1]。然而PCI術后球囊擴張、支架植入及冠脈再灌注損傷內皮細胞、激活冠脈局部炎癥聯級擴大,是PCI術后支架內再狹窄的重要因素[2-3]。替羅非班(Tirofiban)是一種血小板糖蛋白GPⅡb/Ⅲa拮抗劑,具有強效抗血小板聚集作用,預防急性血栓形成,廣泛應用于臨床[4],但給藥途徑仍有爭議。本研究旨在探討替羅非班不同給藥途徑對急診PCI術后患者內皮功能及炎癥因子的影響,為急性心肌梗死臨床治療提供依據,現報道如下。
1 資料與方法
1.1 一般資料 選擇2018年1月-2019年3月本院心血管內科收治的擬行PCI術的急性ST段抬高型心肌梗死患者110例,男65例,女45例;年齡52~78歲,平均(63.2±2.1)歲。納入標準:(1)均符合中華醫學會心血管病學分會《急性ST段抬高型心肌梗死診斷和治療》標準[5];(2)經冠狀動脈造影證實。排除標準:嚴重肝、腎功能障礙;嚴重凝血機制異常;惡性腫瘤;近期有其他活動性出血病史如消化性潰瘍等并發癥;近期重大外傷、腦出血、腦梗死病史;心源性休克、自身免疫性疾病;嚴重的全身其他系統疾病。按隨機數字表法將患者分為對照組55例和觀察組55例。本研究方案經醫院醫學倫理委員會審核通過,所有患者均簽署了知情同意書。
1.2 方法 兩組確診后均予以嚼服阿司匹林腸溶片(生產廠家:拜耳醫藥保健有限公司,批準文號:國藥準字J20171021,規格:100 mg/片),300 mg+硫酸氫氯比格雷片(生產廠家:賽諾菲制藥有限公司,批準文號:國藥準字J20180029,規格:75 mg/片)
300 mg,口服阿托伐他汀片(生產廠家:輝瑞制藥有限公司,批準文號:國藥準字H20051408,規格:20 mg/片)20 mg。對照組術中立即予以替羅非班注射液(生產廠家:魯南貝特制藥有限公司,批準文號:國藥準字H20090328,規格:50 mL︰
12.5 mg)外周靜脈滴注,首次計量為10 μg/kg,再以0.15 μg/(kg·min)經微量注射泵持續靜脈泵入24 h;觀察組于術中予以替羅非班經冠狀動脈內注射用藥,首次用藥劑量為10 μg/kg,再以
0.15 μg/(kg·min)經微量注射泵行持續靜脈注射24 h,術后常規予以低分子肝素注射液(生產廠家:齊魯制藥有限公司,批準文號:國藥準字H20030428,規格:0.2 mL︰2 500 IU)抗凝治療。術后第1天開始口服阿司匹林腸溶片100 mg,1次/d,阿托伐他汀鈣片20 mg,每晚1次;硫酸氫氯比格雷片75 mg,1次/d,根據患者病情需要給予血管緊張素轉化酶抑制劑(ACEI)、β受體阻滯、硝酸酯類藥。
1.3 觀察指標 觀察兩組患者術后1 d和術后1周的CyPA、hs-CRP、MMP-9、NO、vWF、VEGF水平及不良反應發生情況。采用日立全自動生化分析儀以酶聯免疫吸附(ELISA)法檢測CyPA、MMP-9、
hs-CRP、VEGF、vWF,試劑盒購自上海亞培生物科技有限公司,采用硝酸還原酶比色法檢測NO,試劑盒均購自深圳晶美生物工程有限公司。
1.4 統計學處理 采用SPSS 19.0軟件對所得數據進行統計分析,計量資料用(x±s)表示,組間比較采用獨立樣本t檢驗,組內比較采用配對t檢驗;計數資料以率(%)表示,比較采用字2檢驗。以P<0.05為差異有統計學意義。
2 結果
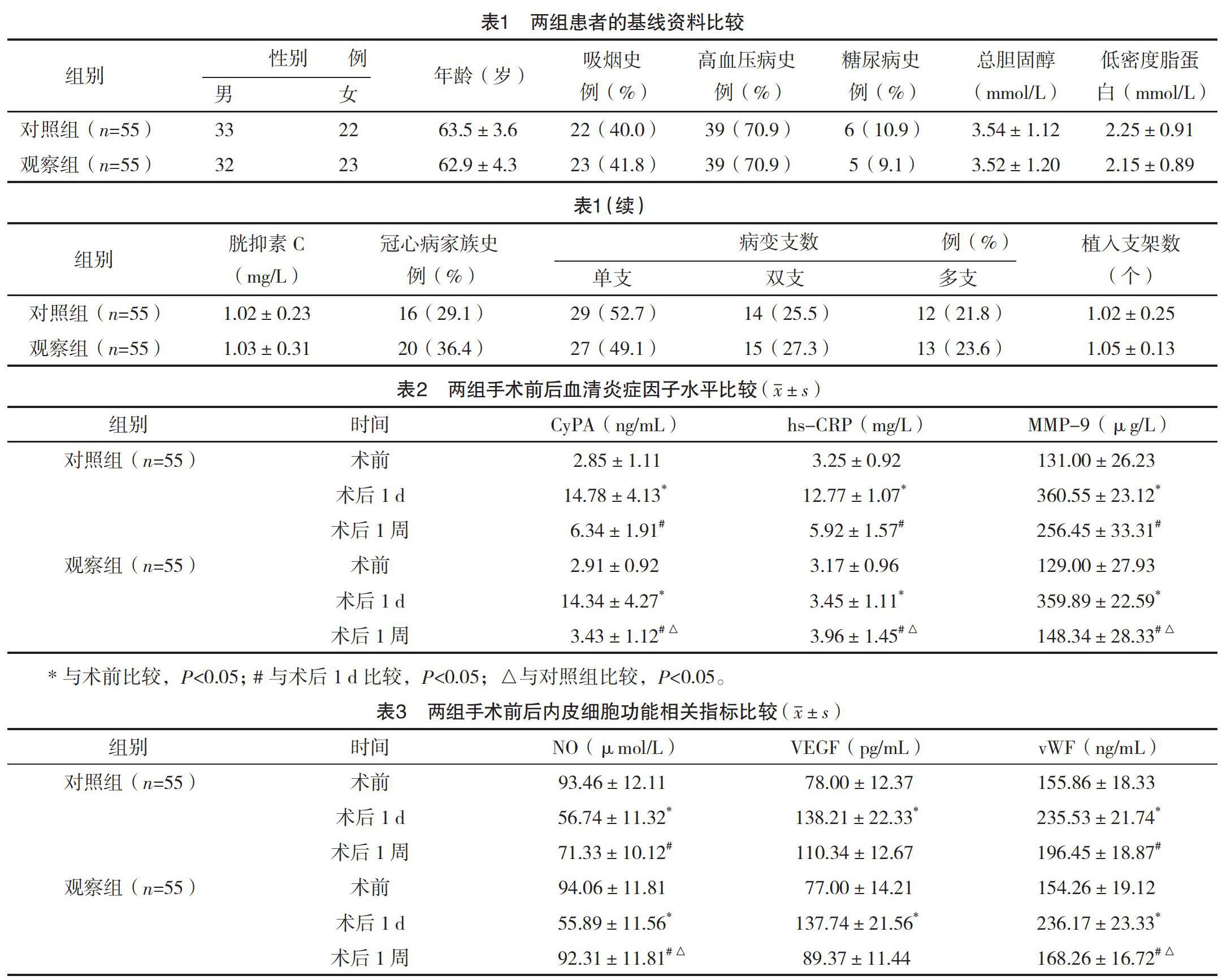
2.1 兩組患者的基線資料比較 兩組患者的性別、年齡、吸煙史等基線資料比較,差異均無統計學意義(P>0.05),具有可比性,見表1。
2.2 兩組手術前后血清炎癥因子水平比較 術前及術后1 d,兩組血清CyPA、hs-CRP、MMP-9比較,差異均無統計學意義(P>0.05);與術前相比,術后1 d,兩組血清CyPA、hs-CRP、MMP-9均明顯升高,差異均有統計學意義(P<0.05);術后1周,兩組血清CyPA、hs-CRP、MMP-9均較術后1 d明顯下降,且觀察組均明顯低于對照組,差異均有統計學意義(P<0.05)。見表2。
2.3 兩組手術前后內皮細胞功能相關指標比
較 術前及術后1 d,兩組血清NO、VEGF、vWF比較,差異均無統計學意義(P>0.05);與術前相比,術后1 d,兩組血清NO濃度均明顯下降,血清VEGF、vWF濃度均明顯上升,差異均有統計學意義(P<0.05);術后1周,兩組血清NO均較術后1 d升高,且觀察組高于對照組,差異均有統計學意義(P<0.05);術后1周,兩組血清VEGF、vWF均較術后1 d下降,且觀察組均低于對照組,差異均有統計學意義(P<0.05)。見表3。
2.4 兩組不良反應發生情況比較 治療期間對照組患者出現頭暈4例、食欲不振3例、皮疹1例、其他2例,不良反應發生率為18.2%;觀察組患者出現頭暈5例、食欲不振2例、皮疹2例、其他1例,不良反應發生率為18.2%。兩組患者治療期間的不良反應發生率比較,差異無統計學意義(P>0.05)。
3 討論
急診PCI術是開通罪犯血管,改善冠狀動脈供血,降低死亡率和改善預后最直接、最有效的方法[5]。但是PCI術中球囊擴展、支架植入等原因損傷內皮細胞、擴大冠狀動脈局部炎癥聯級反應,致使多種炎癥因子及黏附分子表達是最終造成支架內再狹窄的重要原因[6-7]。因此改善PCI術后內皮細胞功能、抑制炎癥反應,對PCI術后患者預后至關重要。
大量研究表明,氧化應激產生活性氧(ROS)誘導血管平滑肌細胞分泌的CyPA,兩者相互影響形成放大效應,誘導炎癥細胞釋放多種炎癥因子、促進平滑肌細胞增生和遷移,參與冠心病發生和發展過程[8];hs-CRP是炎癥反應的非特異性標記物,參與冠心病發展的病理生理過程,PCI術后冠狀動脈內皮細胞損失、局部炎癥因子聯級反應,誘導hs-CRP大量分泌,促進支架內內膜增生,是PCI術后再狹窄重要因素[9];炎癥細胞分泌MMP-9能降解細胞外基質(ECM),誘導粥樣斑塊內血管的生成、血管平滑肌細胞遷移、炎癥細胞聚集,促進冠狀動脈斑塊增長和破裂[10];血管內皮細胞釋放NO具有擴張血管、抑制炎癥細胞黏附、血小板聚集,保證冠狀動脈灌注和微循環,PCI術后內皮細胞功能受損,NO分泌不足,致血管痙攣,加重心肌缺血[11-12];血管內皮細胞缺血、缺氧狀況下分泌大量VEGF,可誘導內皮細胞增生、新生血管形成,改善缺血心肌供血,與心肌缺血程度成正相關[13-17];vWF由血管內皮細胞合成并存儲于內皮細胞之中,血管內皮細胞受損后分泌到血液中參與血栓形成,是血管內皮損傷的特異性標志物之一[18-22]。
替羅非班血小板膜糖蛋白GPⅡb/Ⅲa受體拮抗劑,具有高特異性,可以有效抑制血小板聚集、減輕炎癥反應及改善內皮細胞功能。本研究結果顯示與術前相比,術后1 d,兩組血清CyPA、hs-CRP、MMP-9、VEGF、vWF均明顯升高,血清NO濃度均明顯下降,差異均有統計學意義(P<0.05),提示急性心肌梗死心肌缺血、急診PCI術中球囊擴張、支架植入、再灌注損傷等因素誘發冠狀動脈局部炎癥反應擴大,內皮細胞功能受損。
術后1周,兩組血清CyPA、hs-CRP、MMP-9、VEGF、vWF均較術后1 d明顯下降,血清NO濃度均較術后1 d升高,差異均有統計學意義(P<0.05),提示替羅非班能抑制血小板聚集、改善冠狀動脈微循環、抑制冠狀動脈局部炎癥反應,改善內皮細胞功能。術后1周,觀察組與對照組相比,血清CyPA、hs-CRP、MMP-9、vWF、VEGF下降更明顯,血清NO濃度明顯上升,差異均有統計學意義(P<0.05),提示經冠狀動脈內途徑注入替羅非班較外周靜脈途徑注入替羅非班更能改善急診PCI術后冠狀動脈內皮細胞功能、抑制冠狀動脈局部炎癥反應、改善心臟微循環。
綜上所述,經冠狀動脈內途徑注入替羅非班更能改善急診PCI術后冠狀動脈內皮細胞功能、抑制炎癥反應,改善患者預后,但本研究樣本量較少,此結論有待大樣本,多中心進一步研究證實。
參考文獻
[1] He X,Liu Y,Li Z,et al.Successful Emergency PCI in a Case With AMI Induced by Two-Vessel Spontaneous Coronary Artery Dissection[J].J Interv Cardiol,2015,28(6):609-611.
[2] Masuda J,Kishi M,Kumagai N,et al.Rural-Urban Disparity in Emergency Care for Acute Myocardial Infarction in Japan[J].Circulation Journal,2018,82(6):1666-1674.
[3] Tomilova D I,Byazrova F F,Lopukhova V V,et al.Inflammatory Markers and Their RoIe in Assessing Prognosis of Patients with Stable Coronary Artery Disease after Coronary Stenting[J].Kardiologiia,2015,55(11):88-93.
[4] Ota H,Takehara N,Aonuma T,et al.Association between microalbuminuria predicting in-stent restenosis after myocardial infarction and cellular senescence of endothelial progenitor cells[J].PLoS One,2015,10(4).
[5] Kokkinidis D G,Waldo S W,Armstrong E J.Treatment of coronary artery in-stent restenosis[J].Expert Review of Cardiovascular Therapy,2017,15(3):191-202.
[6]王聰霞,賈珊.冠狀動脈支架內再狹窄發生機制的研究進展[J].西安交通大學學報(醫學版),2018,39(3):303-309.
[7] Johnson N P,Gould K L.Clinical evaluation of a new concept: resting myocardial perfusion heterogeneity quantified by markovian analysis of PET identifies coronary microvascular dysfunction and early atherosclerosis in 1,034 subjects[J].J Nucl Med,2005,46(9):1427-1437.
[8]張優,高傳玉,李牧蔚,等.早期應用替羅非班在急性ST段抬高型心肌梗死擇期經皮冠狀動脈介入治療患者中的療效[J].中華內科雜志,2014,53(4):273-277.
[9] Kim V D H,Gijsen F,Andrew N,et al.The effects of stenting on shear stress: relevance to endothelial injury and repair[J].Cardiovascular Research,2013,99(2):269-275.
[10] Shen Y,Li C,Zhang R Y,et al.Association of increased serum CTRP5 levels with in-stent restenosis after coronary drug-eluting stent implantation: CTRP5 promoting inflammation, migration and proliferation in vascular smooth muscle cells[J].Int J Cardiol,2017,228(1):129-136.
[11] Buccheri D,Piraino D,Andolina G,et al.Understanding and managing in-stent restenosis: a review of clinical data, from pathogenesis to treatment[J].Journal of Thoracic Disease,2016,8(10):1150-1162.
[12] Ohtsuki T,Satoh K,Omura J,et al.Prognostic Impacts of Plasma Levels of Cyclophilin A in Patients with Coronary Artery Disease Highlights[J].Arterioscler Thromb Vasc Biol,2017,37(4):685-693.
[13] Dux C,Lim S C,Jeffree R,et al.Improving nutrition care for neurosurgery patients through a nurse-led transition feeding protocol[J].Nutr Diet,2019,76(2):158-165.
[14] Evans J C,Hirani S P,Needle J J,et al.Nutritional and Post-Transplantation Outcomes of Enteral versus Parenteral Nutrition in Pediatric Hematopoietic Stem Cell Transplantation: A Systematic Review of Randomized and Nonrandomized Studies[J].Biol Blood Marrow Transplant,2019,25(8):252-259.
[15] Tanveer S,Banu S,Jabir N R,et al.Clinical and angiographic correlation of highsensitivity Creactive protein with acute ST elevation myocardial infarction[J].Exp Ther Med,2016,12(6):4089-4098.
[16] Joo W J,Ide K,Kawasaki Y,et al.Effectiveness and safety of early enteral nutrition for patients who received targeted temperature management after out-of-hospital cardiac arrest[J].Resuscitation,2019,135(2):191-196.
[17]劉宇,王新斌.冠狀動脈介入治療前后急性心肌梗死患者基質金屬蛋白酶9與白細胞介素6和P-選擇素水平動態變化的臨床意義[J].中國醫藥,2016,11(10):1438-1441.
[18] Montezano A C,Dulak-Lis M , Tsiropoulou S , et al.Oxidative Stress and Human Hypertension: Vascular Mechanisms, Biomarkers, and Novel Therapies[J].Can J Cardiol,2015,31(5):631-641.
[19] Lerman A.Restenosis: another “dysfunction” of the endothelium[J].Circulation,2005,111(1):8-10.
[20] Kang W K,Lee M H,Kim Y H,et al.Enhanced secretion of biologically active, non-glycosylated VEGF from Saccharomyces cerevisiae[J].Journal of Biotechnology,2013,164(4):441-448.
[21] Li Y,Li L,Dong F,et al.Plasma von Willebrand factor level is transiently elevated in a rat model of acute myocardial infarction[J].Experimental and Therapeutic Medicine,2015,10(5):1743-1749.
[22] Jian-Long M,Jing R,Rui M,et al.High Level of von Willebrand Factor in Non-ST Segment Elevation Myocardial Infarction Patients Predicted Cardiovascular Ischemic Events after Off-Pump Coronary Artery Bypass Surgery[J].International Heart Journal,2015,56(3):298-302.
(收稿日期:2020-07-27) (本文編輯:姬思雨)
猜你喜歡
中國醫學創新(2017年3期)2017-02-22 16:56:52
現代儀器與醫療(2016年6期)2017-01-12 18:26:01
中國當代醫藥(2016年30期)2017-01-07 00:51:21
中國當代醫藥(2016年29期)2017-01-03 23:39:42
中國實用醫藥(2016年30期)2016-12-28 22:58:34
中國實用醫藥(2016年30期)2016-12-28 11:49:52
中國現代醫生(2016年27期)2016-12-21 16:42:20
中國實用醫藥(2016年20期)2016-08-11 21:28:51
中國現代醫生(2015年26期)2016-02-27 12:09:09
山東體育學院學報(2015年3期)2015-08-14 20:33:03