CRP/ALB、PCT與擴展CURB-65評分對老年重癥肺炎的預測價值
2023-04-12 00:00:00胡莎莎常曉青李丹丹李英
現代養生·下半月 2023年3期

【摘要】 " 目的 "探索C反應蛋白與白蛋白比值(CRP/ALB)、降鈣素原(PCT)與擴展英國胸科協會改良肺炎(CURB-65)評分對老年重癥肺炎的預測價值。方法 "收集2020年1月- 2021年12月在河南省人民醫院呼吸與危重癥醫學科就診的老年社區獲得性肺炎104例,根據中國成人社區獲得性肺炎診斷和治療指南(2016版)將患者分為重癥組(47例)與普通組(57例),分析CRP/ALB、PCT與擴展CURB-65評分對老年重癥肺炎的預測價值。結果 "經過單因素及多因素Logistic回歸分析,CRP/ALB、PCT、擴展CURB-65評分與老年重癥肺炎密切相關(Plt;0.05),是老年重癥肺炎的危險因素。ROC曲線分析結果顯示,三項指標均具有預測老年重癥肺炎的作用,但三者并聯試驗,預測效果有所提升。三項指標聯合對老年重癥肺炎的預測結果與實際結果高度一致(Kappa=0.79),并且預測的漏診率和誤診率極低(靈敏度=97.9%,特異度=82.5%),提示三項指標聯合試驗具有較高的臨床應用價值。結論 "CRP/ALB、PCT聯合擴展CURB-65評分對老年重癥肺炎的預測結果與實際結果高度一致,漏測率極低。
【關鍵詞】 "C反應蛋白與白蛋白比值;降鈣素原;擴展英國胸科協會改良肺炎評分;老年重癥肺炎
中圖分類號 "R563.1 " "文獻標識碼 "A " "文章編號 "1671-0223(2023)06--05
Predictive value of CRP/ALB, PCT and expanded CURB-65 score in elderly patients with severe pneumonia "Hu Shasha, Chang Xiaoqing, Li Dandan, Li Ying. Department of Respiratory and Critical Care Medicine, Henan Provincial People's Hospital, Henan University, Zhengzhou 450003, China
【Abstract】 "Objective "To explore the predictive value of C-reactive protein to albumin ratio (CRP/ALB), procalcitonin (PCT) and the expanded CURB-65 score for severe pneumonia in the elderly. Methods "Totally 104 elderly patients with community-acquired pneumonia who visited the Department of Respiratory and Critical Care Medicine of Henan Provincial People's Hospital from January 2020 to December 2021 were collected. According to the Chinese Guidelines for the Diagnosis and Treatment of Adult Community acquired Pneumonia (2016 Edition), the patients were divided into the severe group (47 cases) and the general group (57 cases). The predictive value of CRP/ALB, PCT and expanded CURB-65 for elderly patients with severe pneumonia was analyzed. Results "Through univariate and multivariate Logistic regression analysis, CRP/ALB, PCT and expanded CURB-65 scores were closely related to severe pneumonia in the elderly (Plt;0.05), and were risk factors for severe pneumonia in the elderly. The ROC curve analysis results showed that the three indicators had the function of predicting severe pneumonia in the elderly, but the prediction effect had been improved when the three indicators are tested in parallel. The predicted results of the combination of the three indicators for severe pneumonia in the elderly were highly consistent with the actual results (Kappa=0.79), and the predicted missed diagnosis rate and misdiagnosis rate are extremely low (sensitivity=97.9%, sensitivity=82.5%), suggesting that the combination of the three indicators has high clinical application value. Conclusion "The predicted results of CRP/ALB, PCT combined with expanded CURB-65 score for severe pneumonia in the elderly are highly consistent with the actual results, and the missed test rate is very low.
【Key words】 "C-reactive protein to albumin ratio; Procalcitonin; Expanded CURB-65; Severe pneumonia in the elderly
社區獲得性肺炎(community acquired pneumonia,CAP)指在醫院環境外獲得的急性肺實質感染疾病,它是全球導致免疫功能低下的患者發病和死亡的主要原因之一[1]。入院成人CAP患者平均30天死亡率為4%,重度CAP患者在重癥監護病房(intensive care unit,ICU)平均30天死亡率可能達到23%[2]。CAP的發病率和死亡率隨著年齡的增長而逐漸增加[3]。因此,早期識別老年重癥肺炎尤為重要。近年來,生物標志物在預測CAP嚴重程度的價值受到了廣泛的關注。降鈣素原(procalcitonin,PCT)、C反應蛋白(C-reactive protein,CRP)是經典的評估肺部感染嚴重程度指標。白蛋白(albumin,ALB)被用作感染的預后因素,它傾向于隨著感染的加重而減少[4]。作為基于炎癥和營養的新評分指數,C反應蛋白與白蛋白的比值(C-reactive protein to albumin ratio,CRP/ALB)被證實可預測重癥肺炎所致急性呼吸窘迫綜合征嚴重程度,以及預測膿毒癥預后,但是其預測老年重癥肺炎的相關文獻較少[5-6]。擴展英國胸科協會改良肺炎(confusion,uremia,respiratory,blood pressure and aged 65 years,CURB-65)評分是近年對CAP嚴重程度的評估有著較高的價值的評分系統[7]。本研究通過檢測老年重癥肺炎患者血CRP/ALB、PCT與擴展CURB-65評分,分析其對老年重癥肺炎病情的預測價值,現報告如下。
1 "對象與方法
1.1 "研究對象
選擇2020年1月- 2021年12月醫院呼吸與危重癥醫學科收治的104例老年社區獲得性肺炎患者作為研究對象。納入標準:年齡≥65歲;符合中國成人社區獲得性肺炎診斷和治療指南(2016年版)對CAP及重癥肺炎的診斷標準[8];臨床病例資料完整。排除標準:活動性肺結核患者;惡性腫瘤患者;器官移植患者;免疫抑制患者;中途退出研究者;終末期患者。根據中國成人社區獲得性肺炎診斷和治療指南(2016年版)將104例老年肺炎患者分為重癥組與普通組[8]。重癥組47例,男37例,女10例;年齡65~93歲,中位年齡77(70,84)歲;普通組57例,男29例,女28例;年齡65~94歲,中位年齡72(67,82)歲。研究已獲得醫院倫理委員會審核批準。
1.2 "資料收集
根據醫院電子病歷系統中收集患者基本資料,主要包括年齡、性別、吸煙史、基礎疾病(慢性阻塞性肺疾病、冠心病、高血壓、糖尿病)、呼吸頻率、意識狀態、入院24小時內的白細胞(white blood cell,WBC)計數、淋巴細胞(lymphocyte,LYMP)計數、中性粒細胞(neutrophil,NEU)計數、血小板(platele,PLT)計數、血紅細胞分布寬度(red blood cell distribution width,RDW)計數、PCT、CRP、ALB、纖維蛋白原(fibrinogen,FIB)計數、D-二聚體(d-dimmer)、乳酸脫氫酶、尿素氮等水平,并計算白細胞與淋巴細胞比值(neutrophil lymphocyte ratio,NLR)、CRP/ALB、CURB-65評分及擴展CURB-65評分。
1.3 "數據分析方法
數據采用SPSS 25.0、MedCalc統計學軟件進行數據分析處理。符合正態分布的計量資料以“均數±標準差”表示,組間均數比較進行t檢驗;若不符合正態分布,用“中位數(四分位數間距)”[M(Q1,Q3)]表示,組間中位數比較進行非參數檢驗。計數資料計算百分率,組間率比較進行χ2檢驗。變量間的相關性采用Spearman相關性分析。多因素Logistic 回歸分析用于評估影響老年重癥肺炎的危險因素。采用ROC分析各指標對老年重癥肺炎的預測價值。以Plt;0.05為差異有統計學意義。
2 "結果
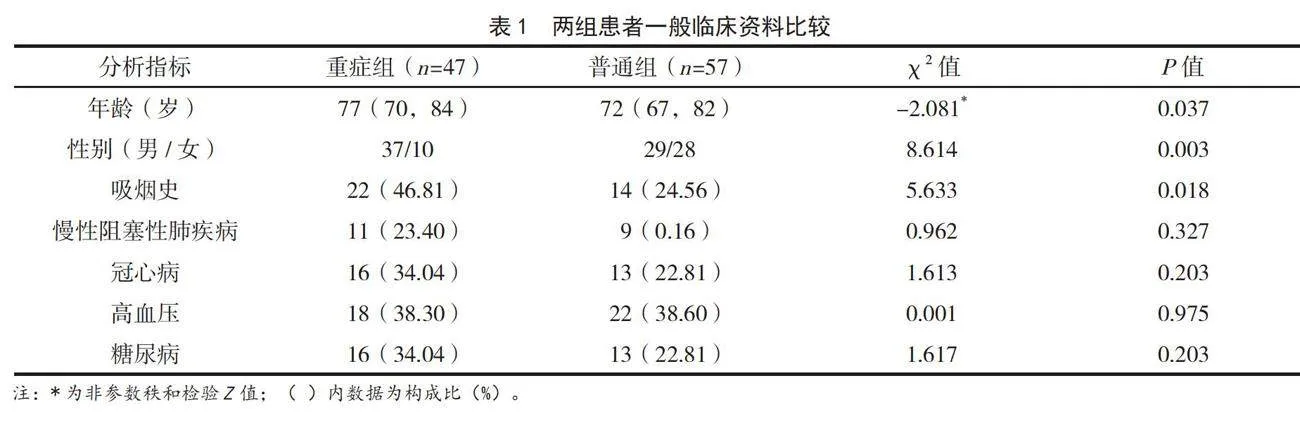
2.1 "重癥組與普通組基礎資料的比較
重癥組與普通組年齡、性別、吸煙史差異有統計學意義(Plt;0.05)。合并慢性阻塞性肺病、冠心病、高血壓、糖尿病等病史在兩組差異無統計學意義(Pgt;0.05)。見表1。
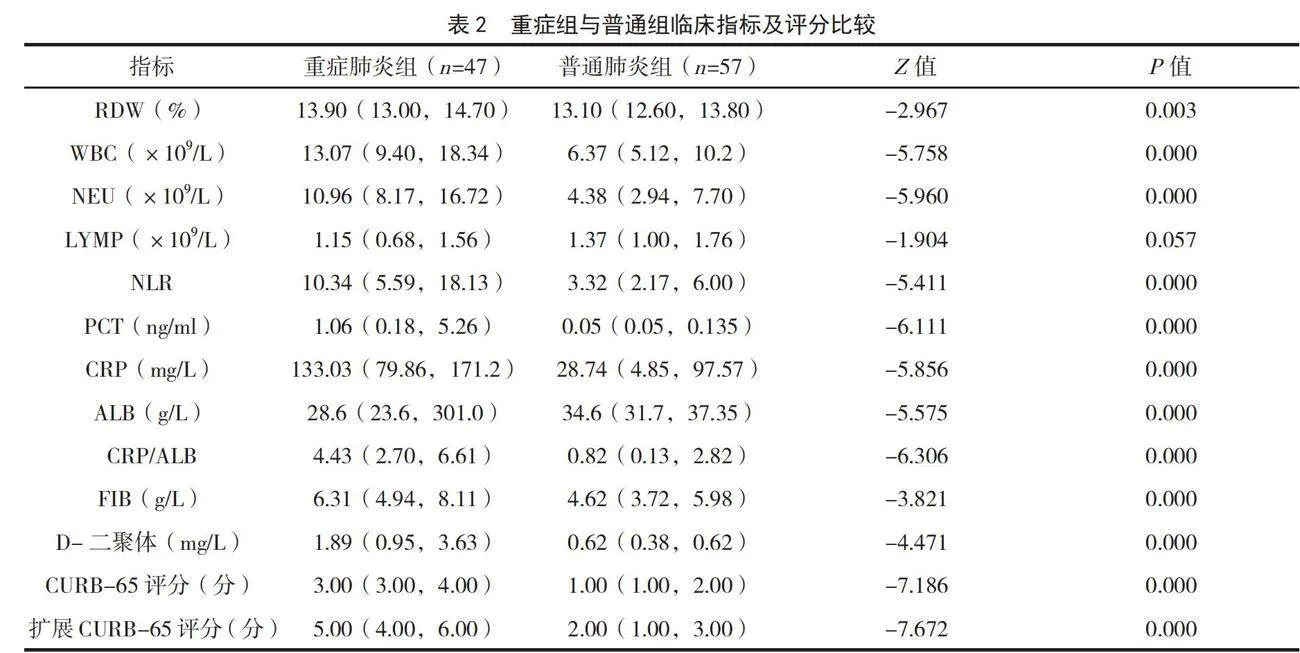
2.2 "兩組臨床指標及CURB-65評分比較
重癥組PCT、CRP/ALB、CRP、RDW計數、WBC計數、NEU計數、NLR、FIB計數、D-二聚體計數、CURB-65評分、擴展CURB-65評分等高于普通組,重癥組的ALB水平低于普通組,差異有統計學意義(Plt;0.05)。重癥組LYMP計數低于普通組,但差異無統計學意義(Pgt;0.05)。見表2。
2.3 "影響老年CAP嚴重程度因素的多因素分析
以是否重度肺炎為因變量(是=1,否=0),上述分析中有統計學意義因素為自變量,進行多因素Logistic回歸分析。結果顯示,CRP/ALB、PCT、ALB、擴展CURB-65評分與老年CAP嚴重程度有關(Plt;0.05),見表3。
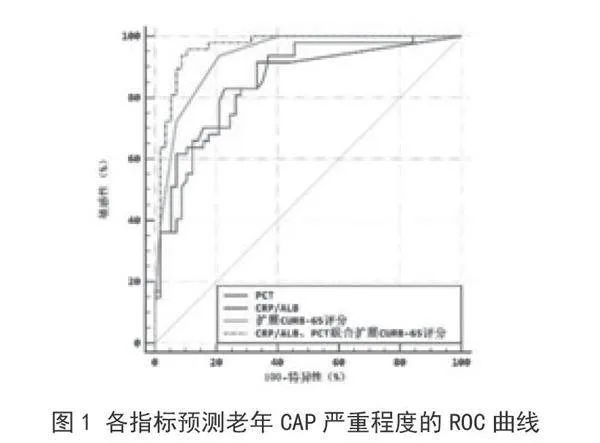
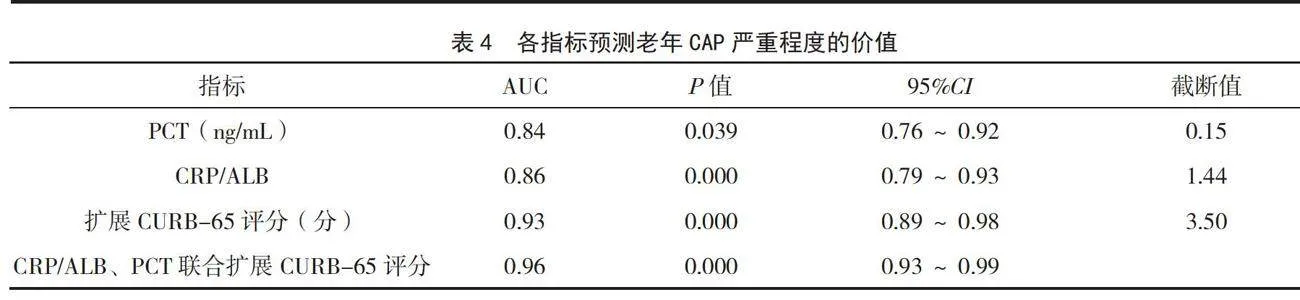
2.4 "各指標預測老年CAP嚴重程度的ROC分析
ROC曲線分析結果顯示,PCT、CRP/ALB及擴展CURB-65評分對老年CAP患者病情嚴重程度均有很好的預測價值,但三者并聯試驗后,曲線下面積有所增大,說明三者聯合試驗可提高預測效能,見表4及圖1。
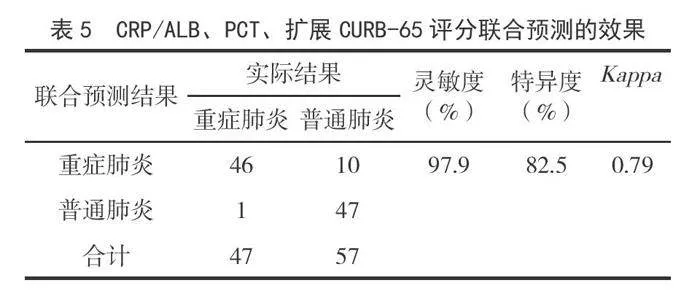
2.5 "三項指標聯合試驗的預測效果
以并聯的方法進行聯合試驗,結果表明,預測結果與實際結果高度一致(Kappa=0.79),并且預測的漏診率和誤診率極低(靈敏度=97.9%,特異度=82.5%),提示三項指標聯合試驗具有較高的臨床應用價值,見表5。
3 "討論
CAP是一種常見的呼吸道疾病,尤其是老年CAP患者經常需要住院治療。CAP可以表現為以發熱、咳嗽、咳痰為特點的輕癥肺炎,也可以表現為有膿毒癥、呼吸衰竭的重癥肺炎[9]。由于病原體和臨床表現的多樣性,如何早期識別老年重癥肺炎是現代養生一大關注點,也是臨床工作中一項挑戰,這對于進一步治療方案的選擇和預測結局也很重要。
生物標志物可用于CAP嚴重程度的早期評估,幫助預測治療反應,并為疾病的病理生理過程提供新的見解[10]。PCT是甲狀腺產生的一種含有116個氨基酸的降鈣素前體,與感染的嚴重程度及器官功能障礙呈正相關[11]。CRP是一種在肝臟中合成的急性期蛋白,已經被證明與肺炎的嚴重程度相關[12]。白蛋白是一種具有重要生理功能的蛋白質,例如維持血漿膠體滲透壓、某些物質的血管內轉運、炎癥反應、血栓形成和脂質代謝[13-15]。CRP、PCT是目前國內外公認的反映CAP嚴重程度的指標,CRP/ALB升高可能是肺炎風險增加之間關系的基礎[16]。CRP/ALB相對簡單且易于在所有環境中使用,它結合了CRP和ALB水平,先前的研究表明,CRP/ALB是預測膿毒癥嚴重程度、危重病及癌癥的預后生物標志物[6,17-18]。本研究結果顯示,在CRP、PCT、WBC、CRP/ALB水平上,老年CAP重癥組高于普通組,并且CRP/ALB在預測老年重癥肺炎的發生方面有較高的參考價值。提示CRP/ALB能作為反映出老年CAP患者的病情嚴重程度的有效指標。
Liu等[7]于2016年提出擴展CURB-65評分系統由8個參數組成,包括意識障礙、尿素>7mmol/L、呼吸頻率≥30次/分鐘、收縮壓<90mmHg或舒張壓≤60mmHg、年齡≥65歲,LDH>230U/L,白蛋白<35g/L,血小板計數<100×109/L,使用擴展CURB-65評分預測CAP患者30天死亡率的價值優于CURB-65評分。本研究結果顯示,擴展CURB-65評分在預測老年CAP患者嚴重程度有較高的價值,且預測能力較CURB-65評分高。并且CRP/ALB、PCT聯合擴展CURB-65評分提高了對老年CAP嚴重程度的預測的準確性。
綜上,CRP/ALB、PCT聯合擴展CURB-65評分對老年重癥肺炎有著較好的預測價值,且指標簡便、容易獲取。
4 "參考文獻
[1] Metlay JP,Waterer GW,Long AC,et al.Diagnosis and treatment of adults with community-acquired pneumonia.An official clinical practice guideline of the american thoracic society and infectious diseases society of America[J].Am J Respir Crit Care Med,2019,200(7):e45-e67.
[2] Restrepo MI,Mortensen EM,Velez JA,et al.A comparative study of community-acquired pneumonia patients admitted to the ward and the ICU[J].Chest,2008,133(3):610-617.
[3] Jain S,Self WH,Wunderink RG,et al.Community-acquired pneumonia requiring hospitalization among U.S.adults[J].N Engl J Med,2015,373(5):415-427.
[4] Arnau-Barres I,Guerri-Fernandez R,Luque S,et al.Serum albumin is a strong predictor of sepsis outcome in elderly patients[J].Eur J Clin Microbiol Infect Dis,2019,38(4):743-746.
[5] 劉海紅.重癥肺炎所致ARDS患者血NT-proBNP、CRP/ALB相關性及聯合預測預后效能分析[J].中國急救復蘇與災害醫學雜志,2021,16(10):1133-1137.
[6] Ranzani OT,Zampieri FG,Forte DN,et al.C-reactive protein/albumin ratio predicts 90-day mortality of septic patients[J].PLoS One,2013,8(3):e59321.
[7] Liu J L,Xu F,Zhou H,et al.Expanded CURB-65:A new score system predicts severity of community-acquired pneumonia with superior efficiency[J].Sci Rep,2016,6:22911.
[8] 中華醫學會呼吸病學分會.中國成人社區獲得性肺炎診斷和治療指南(2016年版)[J].中華結核和呼吸雜志,2016,39(4):253-279.
[9] Aliberti S,Dela Cruz CS,Amati F,et al.Community-acquired pneumonia[J].Lancet,2021,398(10303):906-919.
[10] Fernandez JF,Sibila O,Restrepo MI.Predicting ICU admission in community-acquired pneumonia:Clinical scores and biomarkers[J].Expert Rev Clin Pharmacol,2012,5(4): 445-458.
[11] Guo S,Mao X,Liang M.The moderate predictive value of serial serum CRP and PCT levels for the prognosis of hospitalized community-acquired pneumonia[J].Respir Res,2018,19(1):193.
[12] Chalmers JD,Singanayagam A,Hill AT.C-reactive protein is an independent predictor of severity in community-acquired pneumonia[J].Am J Med,2008,121(3):219-225.
[13] Bernardi M,Angeli P,Claria J,et al.Albumin in decompensated cirrhosis:new concepts and perspectives[J].Gut,2020,69(6):1127-1138.
[14] Rabbani G,Ahn SN.Structure,enzymatic activities,glycation and therapeutic potential of human serum albumin:A natural cargo[J].Int J Biol Macromol,2019,123:979-990.
[15] Arques S.Human serum albumin in cardiovascular diseases[J].Eur J Intern Med,2018,52:8-12.
[16] Kunutsor SK,Laukkanen JA.Serum C-reactive protein-to-albumin ratio is a potential risk indicator for pneumonia:Findings from a prospective cohort study[J].Respir Med,2022,199:106894.
[17] Park JE,Chung KS,Song JH,et al.The C-reactive protein/albumin ratio as a predictor of mortality in critically ill patients[J].J Clin Med,2018,7(10):333.
[18] Luan CW,Yang HY,Tsai YT,et al.Prognostic value of C-reactive protein-to-albumin ratio in head and neck cancer:A meta-analysis[J].Diagnostics(Basel),2021,11(3):403.
[2022-12-10收稿]