抗-HBs聯(lián)合抗-HBe對HBsAg/HBeAg/抗-HBc陽性患者HBeAg血清學(xué)轉(zhuǎn)換的預(yù)測價(jià)值
2023-04-29 18:36:51譚亞峰孫鳳蘭夏巍歐陽耀靈李承彬陳珍霞吳松余運(yùn)運(yùn)江濤
臨床肝膽病雜志 2023年8期
譚亞峰 孫鳳蘭 夏巍 歐陽耀靈 李承彬 陳珍霞 吳松 余運(yùn)運(yùn) 江濤
摘要:目的建立HBsAg/HBeAg/抗-HBc陽性(以下簡稱“大三陽”)+抗-HBe陽性模式患者HBeAg血清學(xué)轉(zhuǎn)換預(yù)測模型,并驗(yàn)證其預(yù)測價(jià)值。方法選取2018年4月1日—2022年8月1日于長江大學(xué)附屬荊州醫(yī)院行乙型肝炎血清標(biāo)志物和HBV DNA定量檢測的乙型肝炎患者6 055例,根據(jù)不同乙型肝炎血清學(xué)指標(biāo)模式分為5組:HBsAg陰性組、HBsAg/抗-HBe/抗-HBc陽性組、大三陽+抗-HBe陽性組、大三陽+抗-HBs陽性組和大三陽組。分析不同乙型肝炎血清學(xué)指標(biāo)模式的特點(diǎn)及不同組別中HBeAg水平的差異。非正態(tài)分布的多組連續(xù)性變量組間比較采用Kruskal-Wallis H檢驗(yàn)。計(jì)數(shù)資料組間比較采用χ2檢驗(yàn)。采用線性回歸分析不同組別HBeAg水平差異。采用Logistic回歸篩選獨(dú)立影響因素,獲得最優(yōu)預(yù)測因子。通過受試者工作特征曲線(ROC曲線)驗(yàn)證預(yù)測效能。使用R Studio4.2.1建立預(yù)測模型并驗(yàn)證。結(jié)果與大三陽模式相比,大三陽+抗-HBe陽性、大三陽+抗-HBs陽性模式患者HBeAg水平均降低(P值均<0.01)。多因素Logistic回歸分析顯示,抗-HBe是HBeAg血清學(xué)轉(zhuǎn)換的獨(dú)立影響因素(P=0.014)。Lasso回歸分析篩選結(jié)果顯示,大三陽+抗-HBe陽性患者發(fā)生HBeAg血清學(xué)轉(zhuǎn)換的最優(yōu)預(yù)測因子為抗-HBe+抗-HBs。ROC曲線結(jié)果顯示,抗-HBe+抗-HBs的AUC為0.733(95%CI: 0.588~0.878,P=0.004 8)。納入抗-HBe+抗-HBs建立預(yù)測模型,其區(qū)分度(AUC=0.733)、準(zhǔn)確度(C=0.733,B=0.20,P=0.946)、檢測效能及穩(wěn)定度(加強(qiáng)Bootstrap檢驗(yàn)C=0.726)均表現(xiàn)良好。結(jié)論乙型肝炎患者體內(nèi)抗-HBs或抗-HBe的出現(xiàn)均促進(jìn)HBeAg水平下降,且抗-HBe促進(jìn)HBeAg水平下降的能力強(qiáng)于抗-HBs。抗-HBe+抗-HBs可用于大三陽+抗-HBe陽性模式患者HBeAg血清學(xué)轉(zhuǎn)換的預(yù)測。
關(guān)鍵詞:乙型肝炎抗原; 血清轉(zhuǎn)換; 預(yù)測
基金項(xiàng)目:荊州市科技計(jì)劃項(xiàng)目(2022HC68)
Predictive value of anti-HBs+anti-HBe for seroconversion of HBeAg in patients with positive?HBsAg/HBeAg/anti-HBc
TAN Yafeng SUN Fenglan XIA Wei OUYANG Yaoling LI Chengbin CHEN Zhenxia WU Song YU Yunyun JIANG Tao(a. Department of Clinical Laboratory, b. Department of Gynecology, Jingzhou Hospital Affiliated to Yangtze?University, Jingzhou, Hubei 434000, China)
Corresponding author:JIANG Tao, jiangtao00358@126.com (ORCID:0000-0002-0852-9190)
Abstract:ObjectiveTo establish a predictive model for HBeAg seroconversion in patients with positive HBsAg/HBeAg/anti-HBc and anti-HBe, and to investigate the predictive value of this model. MethodsA total of 6 055 patients with hepatitis B who received the quantification of the serum markers for hepatitis B and HBV DNA in Jingzhou Hospital Affiliated to Yangtze University from April 1, 2018 to August 1, 2022 were enrolled, and according to the pattern of serological markers for hepatitis B, they were divided into negative HBsAg group, positive HBsAg/anti-HBe/anti-HBc group, positive HBsAg/HBeAg/anti-HBc+positive anti-HBe group, positive HBsAg/HBeAg/anti-HBc+positive anti-HBs group, and positive HBsAg/HBeAg/anti-HBc group. The characteristics of different patterns of serological markers were analyzed, and the level of HBeAg was compared between groups. The Kruskal-Wallis H test was used for comparison of non-normally distributed continuous variables between multiple groups; the chi-square test was used for comparison of categorical data between groups. The linear regression analysis was used to analyze the difference in HBeAg content between different groups; the logistic regression analysis was used to screen for independent influencing factors and obtain the optimal predictive factors. The receiver operating characteristic (ROC) curve analysis was used to validate the predictive performance of the model. R Studio4.2.1 was used to establish and validate the predictive model. ResultsCompared with the positive HBsAg/anti-HBe/anti-HBc group, the positive HBsAg/HBeAg/anti-HBc+positive anti-HBe group and the positive HBsAg/HBeAg/anti-HBc+positive anti-HBs group had a significant reduction in the level of HBeAg? (both P<0.01). The multivariate logistic regression analysis showed that anti-HBe was an independent influencing factor for HBeAg seroconversion (P=0.014), and the Lasso regression analysis showed that anti-HBe+anti-HBs was the optimal predictive factor for HBeAg seroconversion in the patients with positive HBsAg/HBeAg/anti-HBc and positive anti-HBe. The ROC curve analysis showed that anti-HBe+anti-HBs had an area under the ROC curve (AUC) of 0.733 (95% confidence interval: 0.588-0.878, P=0.004 8). Anti-HBe+anti-HBs was included to establish a predictive model, which had good discriminatory ability (AUC=0.733), accuracy (C=0.733, B=0.20, P=0.946), predictive performance, and stability (C=0.726 based on the enhanced Bootstrap test). ConclusionThe presence of anti-HBs or anti-HBe in patients with hepatitis B promotes the reduction in HBeAg level, and anti-HBe had a stronger ability than anti-HBs in promoting such reduction. Anti-HBe+anti-HBs can be used to predict HBeAg seroconversion in patients with positive HBsAg/HBeAg/anti-HBc+positive anti-HBe.
Key words:Hepatitis B Antigens; Seroconversion; Forecasting
Research funding:Jingzhou Science and Technology Plan Project (2022HC68)
成人感染HBV后,大多數(shù)患者可通過自身免疫清除病毒,僅5%~10%的患者發(fā)展為慢性乙型肝炎[1]。HBsAg、HBeAg陽性能夠反映患者體內(nèi)存在病毒復(fù)制,抗-HBs、抗-HBe及抗-HBc是患者免疫應(yīng)答產(chǎn)生的抗體。HBeAg血清學(xué)轉(zhuǎn)換通常是指HBeAg消失后抗-HBe出現(xiàn),是臨床抗病毒治療的重要目標(biāo)之一[2-3]。國內(nèi)外相關(guān)研究顯示,HBsAg/HBeAg/抗-HBc陽性(以下簡稱“大三陽”)乙型肝炎患者HBeAg血清學(xué)轉(zhuǎn)換受病毒及宿主雙方面的影響:(1)病毒方面,HBsAg、HBeAg、HBcrAg、HBV DNA及HBV RNA水平變化對HBeAg血清學(xué)轉(zhuǎn)換有一定的預(yù)測價(jià)值[4-17];宿主方面,抗-HBc及其水平變化對HBeAg血清學(xué)轉(zhuǎn)換也有一定預(yù)測價(jià)值[18-22]。隨著檢測技術(shù)的進(jìn)步,越來越多特殊的乙型肝炎血清學(xué)指標(biāo)模式被發(fā)現(xiàn)[23],包括大三陽+抗-HBe陽性模式和大三陽+抗-HBs陽性模式。目前,鮮有文獻(xiàn)報(bào)道上述特殊模式中抗-HBs、抗-HBe對HBeAg水平的影響,也尚未見有研究探討抗-HBs對乙型肝炎患者HBeAg血清學(xué)轉(zhuǎn)換有無預(yù)測價(jià)值。本研究通過分析不同乙型肝炎血清學(xué)指標(biāo)模式,探討抗-HBs、抗-HBe對HBeAg水平的影響,建立預(yù)測模型,為此類乙型肝炎患者的疾病轉(zhuǎn)歸監(jiān)測提供依據(jù)。
1資料與方法
1.1研究對象選取2018年4月1日—2022年8月1日于長江大學(xué)附屬荊州醫(yī)院行乙型肝炎血清標(biāo)志物和HBV DNA定量檢測的乙型肝炎患者。乙型肝炎診斷標(biāo)準(zhǔn)參照中華醫(yī)學(xué)會(huì)《慢性乙型肝炎防治指南(2019年版)》[2]。排除標(biāo)準(zhǔn):HAV、HCV感染,自身免疫性肝病以及藥物性肝損傷、酒精性肝損傷等。根據(jù)不同的乙型肝炎血清學(xué)指標(biāo)模式,將研究對象分為5組:(1)HBsAg陰性組;(2)HBsAg/抗-HBe/抗-HBc陽性(以下簡稱“小三陽”)組;(3)大三陽+抗-HBe陽性組;(4)大三陽+抗-HBs陽性組;(5)大三陽組。
1.2研究方法
1.2.1觀察指標(biāo)及檢測儀器乙型肝炎血清標(biāo)志物采用HISCL 5000全自動(dòng)化學(xué)發(fā)光法免疫分析儀(日本希森美康公司)檢測;血清HBV DNA定量采用ABI7500實(shí)時(shí)熒光定量聚合酶鏈?zhǔn)椒磻?yīng)(PCR)儀(美國 ABI 公司)檢測;AFP采用Cobas e602全自動(dòng)免疫分析儀(瑞士羅氏公司,Elecsys Ⅱ 定量方法)檢測。肝功能指標(biāo)采用AU5800全自動(dòng)生化分析儀(美國貝克曼庫爾特公司)檢測。所有儀器和試劑經(jīng)過性能驗(yàn)證,均符合ISO15189醫(yī)學(xué)實(shí)驗(yàn)室質(zhì)量及能力認(rèn)證要求。
1.2.2陽性判斷標(biāo)準(zhǔn)(1)血清標(biāo)志物陽性判斷標(biāo)準(zhǔn)為:HBsAg>0.03 IU/mL、抗-HBs>5 mIU/mL、HBeAg>1 COI、抗-HBe>50 抑制率(Inh%)、抗-HBc>1 COI。所有乙型肝炎特殊模式樣本均重復(fù)檢測且通過ELISA方法復(fù)核確認(rèn);HBsAg及抗-HBs為定量檢測,其單位分別為IU/mL及mIU/mL;乙型肝炎血清標(biāo)志物半定量結(jié)果依據(jù)陰性質(zhì)控品(Sysmex)(NC的發(fā)光強(qiáng)度)及陽性質(zhì)控品(Sysmex)(PC的發(fā)光強(qiáng)度)計(jì)算獲得,①HBeAg通過質(zhì)控品的發(fā)光強(qiáng)度計(jì)算臨界值(CO),即CO=(PC的發(fā)光強(qiáng)度-NC的發(fā)光強(qiáng)度)/50+NC的發(fā)光強(qiáng)度;然后計(jì)算檢測樣本的臨界值指數(shù)(COI),即COI=(樣本發(fā)光強(qiáng)度-NC的發(fā)光強(qiáng)度)/(CO-NC的發(fā)光強(qiáng)度),HBeAg>1 COI為陽性。②抗-HBe單位為Inh%,Inh%=(NC的發(fā)光強(qiáng)度-樣本發(fā)光強(qiáng)度)/(NC的發(fā)光強(qiáng)度-PC的發(fā)光強(qiáng)度),抗-HBe>50 Inh%為陽性。③抗-HBc通過質(zhì)控品的發(fā)光強(qiáng)度計(jì)算CO,CO=(PC的發(fā)光強(qiáng)度-NC的發(fā)光強(qiáng)度)/5+NC的發(fā)光強(qiáng)度,然后計(jì)算檢測樣本的COI,COI=(樣本發(fā)光強(qiáng)度-NC的發(fā)光強(qiáng)度)/(CO-NC的發(fā)光強(qiáng)度),HBcAg>1 COI為陽性。(2)HBV DNA臨界值判斷標(biāo)準(zhǔn)為:HBV DNA>2 log10 IU/mL為陽性。血清HBV DNA定量檢測采用實(shí)時(shí)定量PCR法,HBV DNA擴(kuò)增曲線呈“S”形,根據(jù)陽性參考品曲線自動(dòng)換算出HBV DNA載量水平,HBV DNA>2 log10 IU/mL提示HBV DNA陽性,HBV DNA低于檢測下限用0 log10IU/mL表示。(3)AFP臨界值判定標(biāo)準(zhǔn):AFP>7 ng/mL。(4)肝功能臨界值判定標(biāo)準(zhǔn),男性:DBil>9.3 μmol/L、IBil>23.5 μmol/L、TBil>26 μmol/L、Alb<55 g/L、A/G>2.4、Glo>40 g/L、TP>85 g/L、AST>40 U/L、ALT>50 U/L、GGT>60 U/L、ALP>150 U/L;女性:DBil>7.5 μmol/L、IBil>18.9 μmol/L、TBil>21 μmol/L、Alb<55 g/L、A/G>2.4、Glo>40 g/L、TP>85 g/L、AST>35 U/L、ALT>40 U/L、GGT>50 U/L、ALP>150 U/L。
1.3統(tǒng)計(jì)學(xué)方法采用SPSS 26.0軟件進(jìn)行統(tǒng)計(jì)學(xué)分析。計(jì)量資料以M(P25~P75)表示,組間比較采用Kruskal-Wallis H檢驗(yàn)。計(jì)數(shù)資料組間比較采用χ2檢驗(yàn)。采用Logistic回歸篩選獨(dú)立影響因素,增加Lasso(懲罰函數(shù))消除共線性干擾獲得最優(yōu)預(yù)測因子,通過受試者工作特征曲線(ROC曲線)驗(yàn)證預(yù)測效能。使用R4.2.1建立預(yù)測模型并驗(yàn)證。P<0.05為差異有統(tǒng)計(jì)學(xué)意義。
2結(jié)果
2.1一般資料共納入6 055例患者,HBsAg陰性組1 162例,小三陽組3 917例,大三陽+抗-HBe陽性組150例,大三陽+抗-HBs陽性組21例,大三陽組805例。
在大三陽+抗-HBe陽性中篩選出同期行乙型肝炎血清標(biāo)志物、HBV DNA、AFP及肝功能檢測的患者,最終觀察到25例發(fā)生HBeAg 血清學(xué)轉(zhuǎn)換,其中5例獲得HBsAg陰轉(zhuǎn)。本研究根據(jù)25例大三陽+抗-HBe陽性患者HBeAg血清學(xué)轉(zhuǎn)換前后數(shù)據(jù)行單因素、多因素Logistic回歸及Lasso回歸分析,篩選出最優(yōu)預(yù)測因子,應(yīng)用最優(yōu)預(yù)測因子建立大三陽+抗-HBe陽性患者HBeAg血清學(xué)轉(zhuǎn)換的預(yù)測模型并驗(yàn)證。
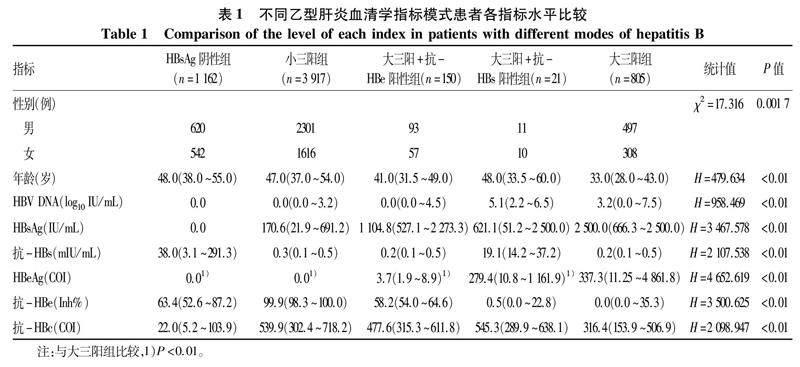
2.2不同乙型肝炎血清學(xué)指標(biāo)模式患者各項(xiàng)指標(biāo)水平比較不同乙型肝炎血清學(xué)指標(biāo)模式患者各項(xiàng)指標(biāo)水平差異均有統(tǒng)計(jì)學(xué)意義(P值均<0.01)(表1)。
2.3不同乙型肝炎血清學(xué)指標(biāo)模式患者HBeAg水平比較分層分析顯示:(1)大三陽+抗-HBs陽性患者由于抗-HBs的出現(xiàn),其HBeAg含量較大三陽組低(P<0.01)。(2)大三陽+抗-HBe陽性患者由于抗-HBe的出現(xiàn),其HBeAg含量較大三陽低(P<0.01)。(3)大三陽+抗-HBe陽性模式患者較大三陽+抗-HBs陽性模式患者HBeAg含量下降的更明顯。(4)大三陽、大三陽+抗-HBs陽性、大三陽+抗-HBe陽性與小三陽4種模式HBeAg水平呈階梯式降低趨勢。
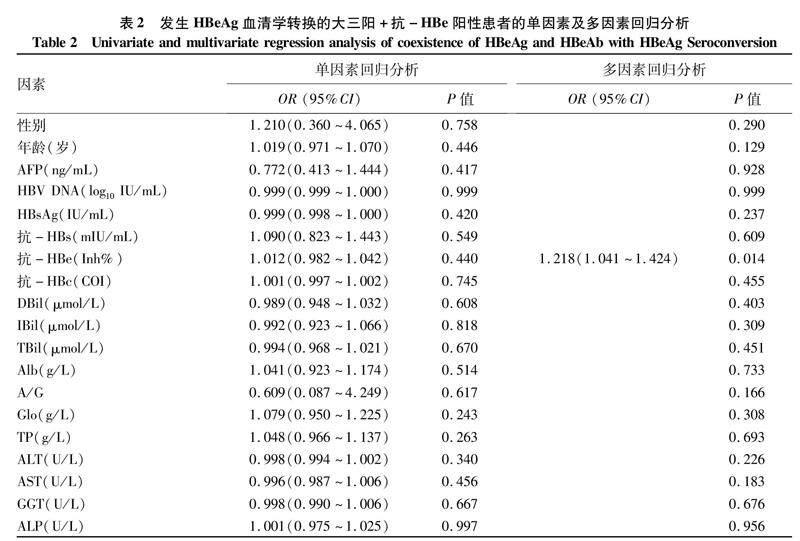
2.4大三陽+抗-HBe陽性患者發(fā)生HBeAg血清學(xué)轉(zhuǎn)換的最優(yōu)預(yù)測因子篩選及驗(yàn)證根據(jù)已出現(xiàn)HBeAg血清學(xué)轉(zhuǎn)換的三陽+抗-HBe陽性患者數(shù)據(jù)進(jìn)行探討,如表2所示,單因素回歸分析顯示,所有觀察指標(biāo)均不是大三陽+抗-HBe陽性患者發(fā)生HBeAg 血清學(xué)轉(zhuǎn)換的獨(dú)立影響因素(P值均>0.05);多因素回歸分析顯示,抗-HBe是HBeAg血清學(xué)轉(zhuǎn)換的獨(dú)立影響因素(P=0.014)。提示抗-HBe在其他因素的協(xié)同作用下可促進(jìn)HBeAg血清學(xué)轉(zhuǎn)換。
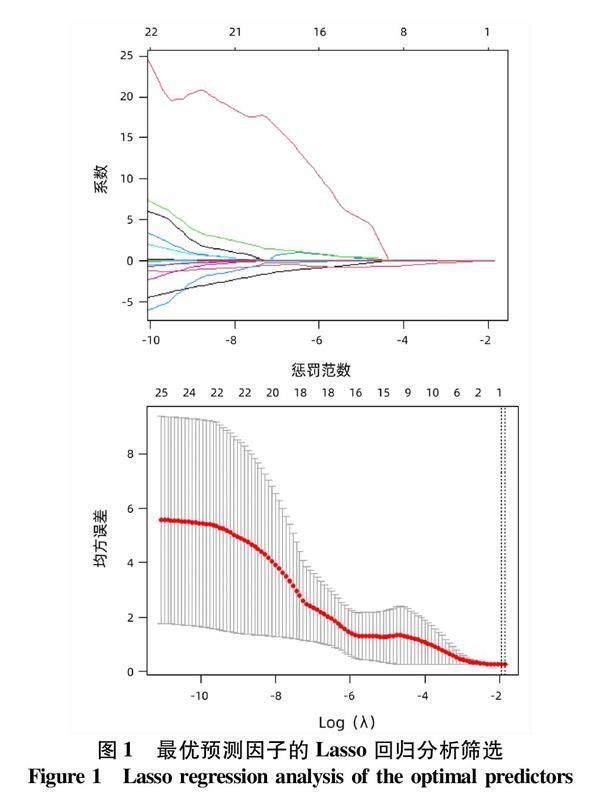
本研究進(jìn)一步增加抗-HBe與抗-HBs、抗-HBc的不同協(xié)同模式及性別、年齡、AFP、HBV DNA、HBsAg、抗-HBs、抗-HBe、抗-HBc、DBil、IBil、TBil、TP、Alb、Glo、A/G、ALT、AST、GGT及ALP均納入Lasso回歸分析,應(yīng)用懲罰函數(shù)消除共線性干擾,最終篩選出促進(jìn)HBeAg血清學(xué)轉(zhuǎn)換最優(yōu)預(yù)測因子為抗-HBe+抗-HBs(圖1)。ROC曲線分析顯示,抗-HBe+抗-HBs預(yù)測大三陽+抗-HBe陽性患者發(fā)生HBeAg血清學(xué)轉(zhuǎn)換的AUC=0.733(95%CI: 0.588~0.878,P=0.004 8)(圖2)。
2.5大三陽+抗-HBe陽性患者發(fā)生HBeAg血清學(xué)轉(zhuǎn)換預(yù)測模型的建立及驗(yàn)證列線圖分析顯示,抗-HBe+抗-HBs是HBeAg血清學(xué)轉(zhuǎn)換的良好預(yù)測指標(biāo)(圖3)。該模型的區(qū)分度良好(AUC=0.733)(圖4a)、準(zhǔn)確度良好(C=0.733,B=0.20,P=0.946)(圖4b)、檢測效能良好(圖4c)及穩(wěn)定度良好(加強(qiáng)Bootstrap檢驗(yàn)C=0.726,檢驗(yàn)曲線與模型校準(zhǔn)曲線貼合良好)(圖4d)。
3討論
抗-HBs、抗-HBe和抗-HBc是患者免疫應(yīng)答過程中產(chǎn)生的抗體,抗-HBc出現(xiàn)最早,抗-HBe常出現(xiàn)于HBeAg消失后,抗-HBs可出現(xiàn)于健康人群疫苗接種后或感染HBV病毒完全康復(fù)后[24]。在臨床實(shí)踐中常見大三陽+抗-HBe陽性和大三陽+抗-HBs陽性模式的患者,其發(fā)生機(jī)制尚不清楚,此特殊模式出現(xiàn)對HBeAg水平的影響以往鮮有文獻(xiàn)報(bào)道。本研究分層分析乙型肝炎不同模式對HBeAg水平的影響,證實(shí)了乙型肝炎患者體內(nèi)抗-HBs或抗-HBe的出現(xiàn)均促進(jìn)HBeAg水平的下降,且抗-HBe促進(jìn)HBeAg水平的下降的效能強(qiáng)于抗-HBs。HBV 炎癥與免疫反應(yīng)相關(guān)研究[25-26]顯示,抗-HBe為依賴T淋巴細(xì)胞介導(dǎo)的特異性抗體,對HBeAg具有較強(qiáng)的中和作用。故本研究認(rèn)為大三陽+抗-HBe陽性患者HBeAg水平下降的原因可能是患者體內(nèi)HBV病毒仍處于高復(fù)制狀態(tài),而體內(nèi)產(chǎn)生的抗-HBe對HBeAg具有一定的清除作用,最終表現(xiàn)為HBeAg水平下降且處于HBeAg與抗-HBe動(dòng)態(tài)平衡狀態(tài)。另有國內(nèi)外多項(xiàng)研究[27-30]顯示,患者發(fā)生HBeAg血清學(xué)轉(zhuǎn)換(HBeAg消失后出現(xiàn)抗-HBe)或HBsAg血清學(xué)轉(zhuǎn)換(HBsAg消失后出現(xiàn)抗-HBs)過程中可觀察到:細(xì)胞因子IL-21水平升高,NK細(xì)胞的活化性受體NKG2D、Toll樣受體表達(dá)上調(diào)及PD-1表達(dá)降低,CD56bright NK細(xì)胞數(shù)量、病毒特異性CD8 T淋巴細(xì)胞數(shù)量增加及調(diào)節(jié)性T淋巴細(xì)胞數(shù)量減少等現(xiàn)象。本研究推測,大三陽+抗-HBs陽性患者HBeAg水平下降的原因可能是患者免疫力較以前增強(qiáng),促進(jìn)了NK細(xì)胞、特異性CD8 T淋巴細(xì)胞數(shù)量的升高及調(diào)節(jié)性T淋巴細(xì)胞數(shù)量減少等而間接增強(qiáng)了機(jī)體清除HBV病毒的能力,從而促使了HBeAg含量下降。但該階段患者體內(nèi)產(chǎn)生的抗-HBs為非HBeAg中和抗體,不能直接中和HBeAg,因此該模式促進(jìn)HBeAg含量下降的效能較大三陽+抗-HBe陽性模式弱。
大三陽+抗-HBe陽性模式出現(xiàn)的原因已有學(xué)者探討,有學(xué)者[31]認(rèn)為是由基因變異引起,即C區(qū)G1896A突變、BCP區(qū)A1762T/G1764A雙突變等,是HBV免疫逃逸的體現(xiàn)。另有學(xué)者[32]認(rèn)為大三陽+抗-HBe陽性是感染了HBV不同亞型導(dǎo)致產(chǎn)生的抗-HBe無法中和體內(nèi)的HBeAg所致。還有學(xué)者[33]指出HBeAg與抗-HBe是患者體內(nèi)病毒復(fù)制和免疫清除動(dòng)態(tài)平衡的體現(xiàn),認(rèn)為大三陽+抗-HBe陽性模式的出現(xiàn)是患者發(fā)生HBeAg血清轉(zhuǎn)化的過渡階段。本研究追溯到25例大三陽+抗-HBe陽性模式患者發(fā)生HBeAg血清學(xué)轉(zhuǎn)換,且有5例獲得HBsAg轉(zhuǎn)陰,驗(yàn)證了大三陽+抗-HBe陽性模式可發(fā)生HBeAg血清學(xué)轉(zhuǎn)換,支持大三陽+抗-HBe陽性模式的出現(xiàn)是患者發(fā)生HBeAg血清學(xué)轉(zhuǎn)換的過渡階段的觀點(diǎn)。
《慢性乙型肝炎防治指南(2019年版)》[2]指出抗-HBe是大三陽患者HBeAg血清學(xué)轉(zhuǎn)換的影響因素,即HBeAg消失后出現(xiàn)抗-HBe為傳統(tǒng)的HBeAg血清學(xué)轉(zhuǎn)換方式。但大三陽+抗-HBe陽性模式HBeAg未消失體內(nèi)便已出現(xiàn)抗-HBe,其能否發(fā)生HBeAg血清學(xué)轉(zhuǎn)換、轉(zhuǎn)化方式是否具有特殊性、有無良好的預(yù)測因子等方面值得深究。本研究驗(yàn)證了大三陽+抗-HBe陽性模式可發(fā)生HBeAg血清學(xué)轉(zhuǎn)換,回歸分析結(jié)果表明,大三陽+抗-HBe陽性模式僅抗-HBe在其他因素的協(xié)同作用下可促進(jìn)HBeAg血清學(xué)轉(zhuǎn)換。本研究增加抗-HBe與其他抗體不同的協(xié)同模式后,將所有影響因素均納入Lasso回歸分析,篩選出最優(yōu)預(yù)測因子為抗-HBe+抗-HBs。ROC曲線分析證實(shí),相較于抗-HBe,抗-HBe+抗-HBs是大三陽+抗-HBe陽性模式發(fā)生HBeAg血清學(xué)轉(zhuǎn)換更優(yōu)的預(yù)測因子,基于抗-HBe+抗-HBs建立的預(yù)測模型,其區(qū)分度、準(zhǔn)確度、檢測效能及穩(wěn)定度均表現(xiàn)良好,可用于此類乙型肝炎患者治療過程的監(jiān)測。
綜上所述,本研究再次證實(shí)了乙型肝炎患者體內(nèi)抗-HBs或抗-HBe的出現(xiàn)均會(huì)促進(jìn)HBeAg水平下降,抗-HBe促進(jìn)HBeAg水平的下降的效能強(qiáng)于抗-HBs,首次探尋出抗-HBe+抗-HBs是大三陽+抗-HBe乙型肝炎患者HBeAg血清學(xué)轉(zhuǎn)換的最優(yōu)預(yù)測因子。但本研究也有局限性:首先,藥物對HBeAg血清學(xué)轉(zhuǎn)換具有一定的影響,拉米夫定、恩替卡韋、阿德福韋酯、替比夫定治療的1年累計(jì)HBeAg血清學(xué)轉(zhuǎn)換率分別為17.24%、13.92%、15.95%和14.04%[8],但本研究未將藥物對HBeAg血清學(xué)轉(zhuǎn)換的影響納入研究模型。其次,HBV基因型及突變對HBeAg血清學(xué)轉(zhuǎn)換也有影響,B型HBV感染的HBeAg血清學(xué)轉(zhuǎn)換率最高,為15.5%,其次為C型7.9%及E型7.4%,1762T/1764A和1862T突變有利于HBeAg血清學(xué)轉(zhuǎn)換[34-36]。而本研究未行基礎(chǔ)實(shí)驗(yàn),未獲得HBV基因型及基因突變等預(yù)測因子的支持。本研究還缺乏多中心研究數(shù)據(jù)支持,未行外部驗(yàn)證。后期筆者團(tuán)隊(duì)將增加基礎(chǔ)實(shí)驗(yàn)并開展廣泛合作,建立多中心數(shù)據(jù)庫進(jìn)行模型開發(fā)與驗(yàn)證。
倫理學(xué)聲明:本研究方案于2022年6月30日經(jīng)由長江大學(xué)附屬荊州醫(yī)院倫理委員會(huì)審批,批號:2022-06-30,所納入患者均簽署知情同意書。利益沖突聲明:本文不存在任何利益沖突。作者貢獻(xiàn)聲明:譚亞峰、孫鳳蘭負(fù)責(zé)課題設(shè)計(jì),資料分析,撰寫論文;夏巍,歐陽耀靈負(fù)責(zé)收集數(shù)據(jù)和統(tǒng)計(jì)分析;李承彬、陳珍霞、吳松負(fù)責(zé)指導(dǎo)數(shù)據(jù)統(tǒng)計(jì)分析;江濤負(fù)責(zé)擬定寫作思路,指導(dǎo)撰寫文章并最后定稿。譚亞峰、孫鳳蘭對本文貢獻(xiàn)等同,同為第一作者。
參考文獻(xiàn):
[1]DUAN MX, GU YN, YU MC, et al. Reasons and clinical significance of HBeAg and anti-HBe double positive in patients with chronic hepatitis B[J]. Chin J Nosocomiology, 2017, 27(19): 4332-4335.段夢夕, 谷婭楠, 于淼琛, 等. 慢性乙型肝炎患者HBeAg與抗-HBe雙陽性的原因與臨床意義[J]. 中華醫(yī)院感染學(xué)雜志, 2017, 27(19): 4332-4335.
[2]Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B (version 2019) [J]. J Clin Hepatol, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.中華醫(yī)學(xué)會(huì)感染病學(xué)分會(huì), 中華醫(yī)學(xué)會(huì)肝病學(xué)分會(huì). 慢性乙型肝炎防治指南(2019年版)[J]. 臨床肝膽病雜志, 2019, 35(12): 2648-2669. DOI: 10.3969/j.issn.1001-5256.2019.12.007.
[3]GU ZY, WANG AH, HE WC, et al. Influencing factors for HBeAg seroconversion in patients with chronic hepatitis B[J]. J Clin Hepatol, 2022, 38(11): 2581-2585. DOI: 10.3969/j.issn.1001-5256.2022.11.029.顧子楊, 王安輝, 何文昌, 等. 慢性乙型肝炎患者HBeAg血清學(xué)轉(zhuǎn)換影響因素的研究進(jìn)展[J]. 臨床肝膽病雜志, 2022, 38(11): 2581-2585. DOI: 10.3969/j.issn.1001-5256.2022.11.029.
[4]YAO CC, LEE CM, HUNG CH, et al. Combining age and HBsAg level predicts post-treatment durability of nucleos(t)ide analogue-induced HBeAg seroconversion[J]. J Gastroenterol Hepatol, 2015, 30(5): 918-924. DOI: 10.1111/jgh.12874.
[5]GISH RG, CHANG TT, LAI CL, et al. Quantitative hepatitis B surface antigen analysis in hepatitis B e antigen-positive nucleoside-naive patients treated with entecavir[J]. Antivir Ther, 2013, 18(5): 691-698. DOI: 10.3851/IMP2559.
[6]ZOULIM F, CAROSI G, GREENBLOOM S, et al. Quantification of HBsAg in nucleos(t)ide-nave patients treated for chronic hepatitis B with entecavir with or without tenofovir in the BE-LOW study[J]. J Hepatol, 2015, 62(1): 56-63. DOI: 10.1016/j.jhep.2014.08.031.
[7]YANG SC, LU SN, LEE CM, et al. Combining the HBsAg decline and HBV DNA levels predicts clinical outcomes in patients with spontaneous HBeAg seroconversion[J]. Hepatol Int, 2013, 7(2): 489-499. DOI: 10.1007/s12072-012-9382-3.
[8]GENG MF, LI YX, GAO FY, et al. A scoring model predicts hepatitis B e antigen seroconversion in chronic hepatitis B patients treated with nucleos(t)ide analogs: Real-world clinical practice[J]. Int J Infect Dis, 2017, 62: 18-25. DOI: 10.1016/j.ijid.2017.06.016.
[9]WANG Y, LIAO H, DENG Z, et al. Serum HBV RNA predicts HBeAg clearance and seroconversion in patients with chronic hepatitis B treated with nucleos(t)ide analogues[J]. J Viral Hepat, 2022, 29(6): 420-431. DOI: 10.1111/jvh.13671.
[10]WANG B, CAREY I, BRUCE M, et al. HBsAg and HBcrAg as predictors of HBeAg seroconversion in HBeAg-positive patients treated with nucleos(t)ide analogues[J]. J Viral Hepat, 2018, 25(8): 886-893. DOI: 10.1111/jvh.12889.
[11]HUANG YJ, CHANG CS, PENG YC, et al. On-treatment HBV DNA level could predict HBeAg seroclearance in patients with HBeAg-positive chronic hepatitis B with entecavir therapy[J]. J Chin Med Assoc, 2017, 80(6): 341-346. DOI: 10.1016/j.jcma.2016.12.005.
[12]PENG CY, HSIEH TC, HSIEH TY, et al. HBV-DNA level at 6 months of entecavir treatment predicts HBeAg loss in HBeAg-positive chronic hepatitis B patients[J]. J Formos Med Assoc, 2015, 114(4): 308-313. DOI: 10.1016/j.jfma.2013.10.023.
[13]JI X, XIA MY, ZHOU B, et al. Serum hepatitis B virus RNA levels predict HBeAg seroconversion and virological response in chronic hepatitis B patients with high viral load treated with nucleos(t)ide analog[J]. Infect Drug Resist, 2020, 13: 1881-1888. DOI: 10.2147/IDR.S252994.
[14]ZHANG M, LI GD, SHANG J, et al. Rapidly decreased HBV RNA predicts responses of pegylated interferons in HBeAg-positive patients: A longitudinal cohort study[J]. Hepatol Int, 2020, 14(2): 212-224. DOI: 10.1007/s12072-020-10015-3.
[15]YE F, ZHAO W, YANG X, et al. The decline of HBV RNA associated with HBeAg seroconversion and double-negative HBV DNA and RNA in chronic hepatitis B patients who received entecavir therapy: a 10-year retrospective cohort study[J].? Ann Transl Med, 2022, 10(16): 897. DOI: 10.21037/atm-22-3265.
[16]LUO H, ZHANG XX, CAO LH, et al. Serum hepatitis B virus RNA is a predictor of HBeAg seroconversion and virological response with entecavir treatment in chronic hepatitis B patients[J]. World J Gastroenterol, 2019, 25(6): 719-728. DOI: 10.3748/wjg.v25.i6.719.
[17]JIA W, ZHU MQ, QI X, et al. Serum hepatitis B virus RNA levels as a predictor of HBeAg seroconversion during treatment with peginterferon alfa-2a[J]. Virol J, 2019, 16(1): 61. DOI: 10.1186/s12985-019-1152-6.
[18]ZHAO XG, WANG J, LIU JC, et al. Baseline serum hepatitis B core antibody level predicts HBeAg seroconversion in patients with HBeAg-positive chronic hepatitis B after antiviral treatment[J]. Antiviral Res, 2021, 193: 105146. DOI: 10.1016/j.antiviral.2021.105146.
[19]WANG CT, ZHANG YF, SUN BH, et al. Models for predicting hepatitis B e antigen seroconversion in response to interferon-α in chronic hepatitis B patients[J]. World J Gastroenterol, 2015, 21(18): 5668-5676. DOI: 10.3748/wjg.v21.i18.5668.
[20]FAN R, SUN J, YUAN Q, et al. Baseline quantitative hepatitis B core antibody titre alone strongly predicts HBeAg seroconversion across chronic hepatitis B patients treated with peginterferon or nucleos(t)ide analogues[J]. Gut, 2016, 65(2): 313-320. DOI: 10.1136/gutjnl-2014-308546.
[21]CAI SH, LI ZD, YU T, et al. Serum hepatitis B core antibody levels predict HBeAg seroconversion in chronic hepatitis B patients with high viral load treated with nucleos(t)ide analogs[J]. Infect Drug Resist, 2018, 11: 469-477. DOI: 10.2147/IDR.S163038.
[22]FU XH, LOU HB, CHEN F, et al. Hepatitis B core antibody and liver stiffness measurements predict HBeAg seroconversion in HBeAg-positive chronic hepatitis B patients with minimally elevated alanine aminotransferase (ALT) levels[J]. Clin Exp Med, 2020, 20(2): 241-248. DOI: 10.1007/s10238-019-00603-5.
[23]XU WZ, TONG YQ, LI Y. Comparison of Roche Elecsys and Sysmex HISCL immunoassays for the screening of common blood-borne pathogens[J]. Ann Transl Med, 2019, 7(14): 300. DOI: 10.21037/atm.2019.05.83.
[24]WIJAYA RS, READ SA, TRUONG NR, et al. HBV vaccination and HBV infection induces HBV-specific natural killer cell memory[J]. Gut, 2021, 70(2): 357-369. DOI: 10.1136/gutjnl-2019-319252.
[25]TSUKUDA S, WATASHI K. Hepatitis B virus biology and life cycle[J]. Antiviral Res, 2020, 182: 104925. DOI: 10.1016/j.antiviral.2020.104925.
[26]KEENAN BP, FONG L, KELLEY RK. Immunotherapy in hepatocellular carcinoma: The complex interface between inflammation, fibrosis, and the immune response[J]. J Immunother Cancer, 2019, 7(1): 267. DOI: 10.1186/s40425-019-0749-z.
[27]CHEN T, ZHU L, SHI AC, et al. Functional restoration of CD56bright NK cells facilitates immune control via IL-15 and NKG2D in patients under antiviral treatment for chronic hepatitis B[J]. Hepatol Int, 2017, 11(5): 419-428. DOI: 10.1007/s12072-017-9803-4.
[28]HU X, MA S, HUANG X, et al. Interleukin-21 is upregulated in hepatitis B-related acute-on-chronic liver failure and associated with severity of liver disease[J]. J Viral Hepat, 2011, 18(7): 458-467. DOI: 10.1111/j.1365-2893.2011.01475.x.
[29]YANG JZ, SHENG GP, XIAO DS, et al. The frequency and skewed T-cell receptor beta-chain variable patterns of peripheral CD4(+)CD25(+) regulatory T-cells are associated with hepatitis B e antigen seroconversion of chronic hepatitis B patients during antiviral treatment[J]. Cell Mol Immunol, 2016, 13(5): 678-687. DOI: 10.1038/cmi.2015.100.
[30]XIA J, HUANG R, CHEN YX, et al. Profiles of serum soluble programmed death-1 and programmed death-ligand 1 levels in chronic hepatitis B virus-infected patients with different disease phases and after anti-viral treatment[J]. Aliment Pharmacol Ther, 2020, 51(11): 1180-1187. DOI: 10.1111/apt.15732.
[31]AN X, LIU SH, XIA LN, et al. Efficacy and clinical outcomes of different antiviral regimens in HBeAg/HBeAb double-positive patients with chronic hepatitis B[J]. J Army Med Univ, 2022, 44(2): 162-167. DOI: 10.16016/j.2097-0927.202107114.安選, 劉書宏, 夏莉娜, 等. HBeAg/HBeAb雙陽性慢性乙型肝炎患者不同抗病毒方案療效及臨床轉(zhuǎn)歸分析[J]. 陸軍軍醫(yī)大學(xué)學(xué)報(bào), 2022, 44(2): 162-167. DOI: 10.16016/j.2097-0927.202107114.
[32]LUO L, ZHANG TC, LIU SG. Clinical characteristics of chronic hepatitis B patients with both HBeAg and HBeAb positive[J]. J Mol Diagn Ther, 2019, 11(5): 387-390, 433. DOI: 10.3969/j.issn.1674-6929.2019.05.011.羅琳, 張廷超, 劉書剛. HBeAg與抗-HBe雙陽性的慢性乙型肝炎患者臨床特征分析[J]. 分子診斷與治療雜志, 2019, 11(5): 387-390, 433. DOI: 10.3969/j.issn.1674-6929.2019.05.011.
[33]WANG H, WANG HP, QIAN LY, et al. Maternal breast feeding safety of hepatitis B virus carrying parturient women with hepatitis B surface antigen and hepatitis B e antigen double positive[J]. Chin J Infect Dis, 2020, 38(1): 44-48. DOI: 10.3760/cma.j.issn.1000-6680.2020.01.006.王虹, 王紅萍, 錢琳妍, 等. 乙型肝炎表面抗原和乙型肝炎e抗原雙陽性的乙型肝炎病毒攜帶產(chǎn)婦進(jìn)行母乳喂養(yǎng)的安全性[J]. 中華傳染病雜志, 2020, 38(1): 44-48. DOI: 10.3760/cma.j.issn.1000-6680.2020.01.006.
[34]KAO JH, CHEN PJ, LAI MY, et al. Hepatitis B virus genotypes and spontaneous hepatitis B e antigen seroconversion in Taiwanese hepatitis B carriers[J]. J Med Virol, 2004, 72(3): 363-369. DOI: 10.1002/jmv.10534.
[35]SHIMAKAWA Y, LEMOINE M, NJAI HF, et al. Natural history of chronic HBV infection in West Africa: A longitudinal population-based study from The Gambia[J]. Gut, 2016, 65(12): 2007-2016. DOI: 10.1136/gutjnl-2015-309892.
[36]KRAMVIS A, KOSTAKI EG, HATZAKIS A, et al. Immunomodulatory function of HBeAg related to short-sighted evolution, transmissibility, and clinical manifestation of hepatitis B virus[J]. Front Microbiol, 2018, 9: 2521. DOI: 10.3389/fmicb.2018.02521.
收稿日期:2022-12-02;錄用日期:2023-01-09
本文編輯:邢翔宇
引證本文:TAN YF, SUN FL, XIA W,? et al. Predictive value of anti-HBs+anti-HBe for? seroconversion of HBeAg in patients with positive HBsAg/HBeAg/anti-HBc[J]. J Clin Hepatol, 2023, 39(8): 1832-1840.
