手術病人術后自控鎮痛的療效觀察
2024-07-05 22:47:32馬麗芳陳曉霞陳英
循證護理 2024年12期
關鍵詞:護理
馬麗芳 陳曉霞 陳英


Observation on the efficacy of operating patient controlled analgesia after operation
MA Lifang,CHEN Xiaoxia,CHEN YingLanzhou University Second Hospital,Gansu 730030 ChinaCorresponding Author MA Lifang,E-mail:malifang2023@163.com
Keywords patient controlled analgesia;postoperation;pain;anesthesia;nursing
摘要 目的:觀察病人自控鎮痛(PCA)對手術后急性疼痛的療效和安全性。方法:對2021年1月—2023年3月在蘭州大學第二醫院行手術治療并于麻醉恢復室轉運的病人臨床資料進行回顧性研究;根據病人出麻醉室時是否攜帶PCA分為兩組,比較兩組病人術后24 h和48 h的視覺疼痛評分(VAS)及惡心、干嘔、嘔吐、頭暈和頭痛的發生率。結果:結果顯示,攜帶PCA的病人于術后24 h(χ 2=1 099.1,P<0.001)和48 h(χ 2=2 146.5,P<0.001)均表現出更低的VAS評分,而兩組病人的惡心(χ 2=1.600,P>0.05)、干嘔(χ 2=2.011,P>0.05)、嘔吐(χ 2=2.131,P>0.05)、頭暈(χ 2=2.732,P>0.05)及頭痛(χ 2=1.267,P>0.05)的發生率比較差異均無統計學意義。結論:PCA可以減輕手術后病人24 h和48 h的急性疼痛,并且沒有增加麻醉相關不良反應,是加速康復外科及增加護理滿意度的理想鎮痛方式。
關鍵詞 病人自控鎮痛;術后;疼痛;麻醉;護理
doi:10.12102/j.issn.2095-8668.2024.12.037
外科手術病人多會經歷急性術后疼痛。有證據表明,僅有不到一半的病人術后疼痛得到緩解[1],許多病人對其疼痛管理高度不滿[2]。急性疼痛治療不當會造成許多短期和長期的后果,如高血糖、胰島素抵抗、增加感染風險,甚至導致慢性疼痛[3-4]。因此,更好的疼痛管理可以提升病人對護理的滿意度[5],并更有助于加速康復外科的實施。病人自控鎮痛(patient controlled analgesia,PCA)的創始人之一Sechzer認為,“如果病人能夠對疼痛和焦慮有更多的自主控制權,這樣會使他們應用更少的藥物”[6],其在20世紀60年代把PCA引入臨床[7],使病人能自主地施用預定劑量的鎮痛劑,該特定劑量由專業醫護人員設定,并且限制在特定時間間隔內施用一定劑量或限制累積劑量[8]。PCA常使用阿片類藥物、非甾體抗炎藥(nonsteroidal antiinflammatory drugs,NSAIDs)或局部麻醉藥,通過靜脈內、硬膜外、皮下及鼻腔途徑給藥,常用于急性術后疼痛的鎮痛,也可用于其他類型的急性疼痛管理[8]。但是PCA存在侵入性、限制病人移動、需要攜帶靜脈管道、參數設置錯誤所致的安全性問題[9-10]及麻醉藥的不良反應等[11-13]局限,本研究通過調查術后攜帶PCA與未攜帶PCA病人的疼痛緩解情況以及不良反應,評價PCA的鎮痛效果及安全性,進一步評價其臨床應用價值。
1 對象與方法
1.1 研究對象
選擇2021年1月—2023年3月在蘭州大學第二醫院麻醉手術科經麻醉恢復室轉運的病人為研究對象。納入標準:1)年齡18~65歲;2)圍術期生命體征平穩;3)病人依從性較好。排除標準:1)兒童;2)頭頸部手術者;3)美國麻醉醫師協會(ASA)分級≥Ⅲ級;4)肝腎功能異常、精神疾病或意識障礙者;5)存在阿片類藥物濫用史;6)麻醉劑過敏;7)慢性阻塞性肺疾病及顱內壓增高者。本研究最終納入41 533例手術病人,其中17 168例病人出麻醉室后攜帶了PCA,24 365例病人出麻醉室后未攜帶PCA。
1.2 調查方法
1)疼痛視覺模擬評分(Visual Analogue Scale,VAS):評估攜帶PCA和未攜帶PCA的兩組病人術后24 h和48 h的疼痛情況,其中0分表示無痛,1~3分表示輕微疼痛,4~6分表示中度疼痛,7~10分表示重度疼痛[14]。2)術后并發癥:統計兩組病人術后惡心、干嘔、嘔吐、頭暈及頭痛的發生情況。
1.3 資料收集方法
術前1 d病人簽署麻醉知情同意書,并向病人告知PCA的用途及不良反應,病人自行決定是否術后攜帶PCA。攜帶PCA者于術后停止麻醉維持藥物后安裝PCA,PCA參數為:維持量2 mL/h,每次自控劑量0.5 mL,鎖定時間15 min,PCA藥物使用0.9%氯化鈉注射液配制。分別于術后24 h和48 h對病人進行VAS評估,并于術后48 h詢問病人有無惡心、干嘔、嘔吐、頭暈及頭痛等并發癥,然后對收集結果進行匯總。
1.4 統計學方法
采用SPSS 26.0軟件進行統計分析。定量資料采用均數±標準差(x±s)表示,組間比較采用t檢驗,定性資料采用例數和百分比(%)表示,組間比較采用χ 2檢驗。以P<0.05為差異有統計學意義。
2 結果
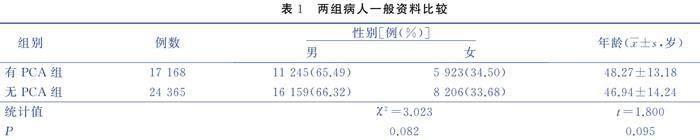
2.1 一般資料
兩組病人的性別和年齡差異均無統計學意義,表明術后攜帶PCA與未攜帶PCA的病人之間具有可比性。見表1。
2.3 兩組病人不良反應發生率比較(見表3)
3 討論
自1971年以來,PCA被用于緩解疼痛,第一個商用PCA泵于1976年誕生,允許病人按下按鈕,按需施用預定推注劑量的藥物來緩解疼痛[15]。PCA可用于治療急性、慢性、術后和分娩疼痛[16]。通常使用阿片類藥物和局部麻醉劑,偶有其他類型鎮痛藥。這些藥物一般通過靜脈內、硬膜外、外周神經導管或經皮給藥[17-18]。且PCA更有利于術后疼痛的控制,易獲得病人更高的滿意度[19]。盡管當前的研究證實了PCA的鎮痛效果,但仍然需要更多的研究評估該疼痛管理策略的安全性和有效性[20-21]。
本研究結果發現,手術后攜帶PCA有助緩解病人疼痛,且并沒有引起更多的麻醉相關不良反應,肯定了其術后鎮痛效果及安全性。本研究同樣存在一定局限性,如本研究為回顧性調查,且病人不是隨機分配的,未分析手術方式和手術部位對研究結果的影響;由于樣本量較大,收集部分術前信息較困難,從而缺乏術前信息。但目前大多數關于PCA的臨床研究樣本均較小[22-25],使證據價值推廣受限。本研究的優勢在于調查的病人數量較多;此外,術后24 h和48 h是急性疼痛恢復的黃金時間,疼痛通常在術后24 h內更明顯[21]。本研究對術后第2個24 h進行了評價,以排除第1個24 h存在的術中麻醉的影響。
4 小結
本研究肯定了PCA對疼痛緩解的有效性和安全性。未來可進一步探索PCA對不同疾病、不同手術方式、不同手術部位的鎮痛效果,以及不同鎮痛藥物是否有不同的鎮痛效果,以幫助臨床中制定個性化PCA疼痛管理方案,從而提高病人的滿意度。
參考文獻:
[1] APFELBAUM J L,CHEN C,MEHTA S S,et al.Postoperative pain experience:results from a national survey suggest postoperative pain continues to be undermanaged[J].Anesthesia and Analgesia,2003,97(2):534-540.
[2] BENHAMOU D,BERTI M,BRODNER G,et al.Postoperative analgesic therapy observational survey (PATHOS):a practice pattern study in 7 central/southern European countries[J].Pain,2008,136(1/2):134-141.
[3] SINATRA R.Causes and consequences of inadequate management of acute pain[J].Pain Medicine,2010,11(12):1859-1871.
[4] PERGOLIZZI J V Jr,RAFFA R B,TAYLOR R Jr.Treating acute pain in light of the chronification of pain[J].Pain Management Nursing,2014,15(1):380-390.
[5] SCHWENKGLENKS M,GERBERSHAGEN H J,TAYLOR R S,et al.Correlates of satisfaction with pain treatment in the acute postoperative period:results from the international pain out registry[J].Pain,2014,155(7):1401-1411.
[6] SECHZER P H.Studies in pain with the analgesic-demand system[J].Anesthesia & Analgesia,1971,50(1):1-10.
[7] SECHZER P H.Objective measurement of pain[C].American:The American Society of Anesthesiologist,1968,29(1):209-210.
[8] GRASS J A.Patient-controlled analgesia[J].Anesthesia and Analgesia,2005,101(5 Suppl):S44-S61.
[9] SCHUG S A,PALMER G M,SCOTT D A,et al.Acute pain management:scientific evidence,fourth edition,2015[J].The Medical Journal of Australia,2016,204(8):315-317.
[10] AHMAD I,THOMPSON A,FRAWLEY M,et al.Five-year experience of critical incidents associated with patient-controlled analgesia in an Irish University Hospital[J].Irish Journal of Medical Science,2010,179(3):393-397.
[11] MORLION B,SCHFER M,BETTERIDGE N,et al.Non-invasive patient-controlled analgesia in the management of acute postoperative pain in the hospital setting[J].Current Medical Research and Opinion,2018,34(7):1179-1186.
[12] CHELLY J E,GRASS J,HOUSEMAN T W,et al.The safety and efficacy of a fentanyl patient-controlled transdermal system for acute postoperative analgesia:a multicenter,placebo-controlled trial[J].Anesthesia and Analgesia,2004,98(2):427-433.
[13] GROND S,HALL J,SPACEK A,et al.Iontophoretic transdermal system using fentanyl compared with patient-controlled intravenous analgesia using morphine for postoperative pain management[J].British Journal of Anaesthesia,2007,98(6):806-815.
[14] OLSZEWSKI P K,MCCOLL L K,HERISSON F M,et al.Blunted hyperphagic and c-Fos immunoreactivity responsiveness to an orexigen,butorphanol tartrate,in aged rats[J].Neuroscience Letters,2019,711:134409.
[15] PASTINO A,LAKRA A.Patient controlled analgesia[M].Treaure Island:StatPearls,2023:1.
[16] MANN C,OURO-BANG′NA F,ELEDJAM J J.Patient-controlled analgesia[J].Current Drug Targets,2005,6(7):815-819.
[17] AGUIRRE J,DEL MORAL A,COBO I,et al.The role of continuous peripheral nerve blocks[J].Anesthesiology Research and Practice,2012,2012:560879.
[18] VISCUSI E R,REYNOLDS L,CHUNG F,et al.Patient-controlled transdermal fentanyl hydrochloride vs intravenous morphine pump for postoperative pain:a randomized controlled trial[J].JAMA,2004,291(11):1333-1341.
[19] MCNICOL E D,FERGUSON M C,HUDCOVA J.Patient controlled opioid analgesia versus non-patient controlled opioid analgesia for postoperative pain[J].The Cochrane Database of Systematic Reviews,2015,2015(6):CD003348.
[20] NIJLAND L,SCHMIDT P,FROSCH M,et al.Subcutaneous or intravenous opioid administration by patient-controlled analgesia in cancer pain:a systematic literature review[J].Supportive Care in Cancer,2019,27(1):33-42.
[21] CHEN X H,YAO J Z,XIN Y R,et al.Postoperative pain in patients undergoing cancer surgery and intravenous patient-controlled analgesia use:the first and second 24 h experiences[J].Pain and Therapy,2023,12(1):275-292.
[22] LIN R B,LIN S Z,FENG S T,et al.Comparing patient-controlled analgesia versus non-PCA hydromorphone titration for severe cancer pain:a randomized phase Ⅲ trial[J].Journal of the National Comprehensive Cancer Network,2021,19(10):1148-1155.
[23] XU J H,PU M T,XU X,et al.The postoperative analgesic effect of intercostal nerve block and intravenous patient-controlled analgesia on patients undergoing lung cancer surgery[J].American Journal of Translational Research,2021,13(8):9790-9795.
[24] AYDIN O N,KIR E,OZKAN S B,et al.Patient-controlled analgesia and sedation with fentanyl in phacoemulsification under topical anesthesia[J].Journal of Cataract and Refractive Surgery,2002,28(11):1968-1972.
[25] LUAN H F,ZHANG X B,FENG J Y,et al.Effect of dexmedetomidine added to ropivacaine on ultrasound-guided transversus abdominis plane block for postoperative analgesia after abdominal hysterectomy surgery:a prospective randomized controlled trial[J].Minerva Anestesiologica,2016,82(9):981-988.
(本文編輯趙奕雯 孫玉梅)
作者簡介 馬麗芳,主管護師,本科,E-mail:malifang2023@163.com
引用信息 馬麗芳,陳曉霞,陳英.手術病人術后自控鎮痛的療效觀察[J].循證護理,2024,10(12):2275-2277.
猜你喜歡
安徽醫學(2022年10期)2022-11-12 02:42:20
醫學食療與健康(2021年27期)2021-05-13 18:46:23
醫學概論(2021年18期)2021-01-21 22:46:45
中華養生保健(2020年7期)2020-11-16 01:14:02
中華養生保健(2020年3期)2020-11-16 00:52:46
中華養生保健(2020年2期)2020-11-16 00:49:54
家庭醫學(下半月)(2019年9期)2019-10-12 08:04:18
經濟技術協作信息(2018年20期)2019-01-19 02:56:26
中國衛生(2016年2期)2016-11-12 13:22:32
中國中醫藥現代遠程教育(2014年20期)2014-03-01 04:31:38