RhoB和E-cadherin在非小細胞肺癌組織中的表達及臨床意義
2014-06-05 15:31:00譚祎媚徐美林徐醫軍
天津醫藥 2014年1期
譚祎媚 張 遜 徐美林 王 菁 徐醫軍
RhoB和E-cadherin在非小細胞肺癌組織中的表達及臨床意義
譚祎媚1張 遜2△徐美林3王 菁3徐醫軍2
目的探討非小細胞肺癌(NSCLC)中RhoB和E-鈣黏蛋白(E-cadherin)的表達及其臨床意義。方法采用免疫組化Super Pic TureTMPolymer二步法,檢測116例NSCLC組織(NSCLC組)和同期116例正常余肺組織(正常組)中RhoB和E-cadherin的表達,并分析其表達與患者臨床病理特征及預后的關系。結果NSCLC組RhoB、E-cadherin陽性表達率均低于正常組(57.76%vs 87.07%,54.31%vs 85.34%,均P<0.01)。NSCLC組織中RhoB的表達強度在不同腫瘤病理類型、腫瘤分化程度及淋巴結轉移情況間的差異有統計學意義,E-cadherin的表達強度在不同TNM分期、腫瘤分化程度及淋巴結轉移情況間的差異有統計學意義。NSCLC組RhoB與E-cadherin的表達呈正相關(r= 0.503,P<0.01)。RhoB高表達的患者3年生存率高于低表達者(83.93%vs 40.00%,Log-rank χ2=18.992,P<0.01);E-cadherin高表達的患者3年生存率高于低表達者(85.11%vs 44.93%,Log-rank χ2=16.680,P<0.01)。RhoB和E-cadherin共同低表達、淋巴結轉移是影響NSCLC患者預后的危險因素。結論RhoB與E-cadherin在NSCLC組織中的表達呈現較好的相關性,檢測二者的表達對判斷NSCLC患者的臨床病理學特征及預后有一定提示作用。
癌,非小細胞肺;鈣黏著糖蛋白類;免疫組織化學;預后;Kaplan-Meiers評估;RhoB;E-鈣黏蛋白
肺癌中85%為非小細胞肺癌(non-small cell lung cancer,NSCLC),大量研究證明,NSCLC的侵襲與轉移是造成其不良預后的主要原因[1]。Rho亞家族成員RhoB在腫瘤發生過程中是一個負調節因子,具有抑制某些腫瘤細胞增殖、上調細胞凋亡以及抑制炎癥反應的作用[2]。E-鈣黏蛋白(E-cadherin)是分布在所有上皮組織中的跨膜糖蛋白,它具有促進上皮細胞間相互黏附、保持組織結構完整性的作用[3]。肺癌組織中RhoB、E-cadherin的表達及其與患者臨床病理特征的關系已有相關研究,但其與患者預后關系的臨床報道不多。本研究采用免疫組化法檢測NSCLC組織及正常肺組織中RhoB、E-cadherin蛋白的表達,探討其與NSCLC患者臨床病理特征及預后的關系。
1 資料與方法
1.1 研究對象及標本來源 選取天津市胸科醫院2008年1月—12月NSCLC患者116例(NSCLC組),其中男85例,女31例。年齡32~78歲,平均(60.38±9.84)歲;所有病例均經病理證實,術前未經過放化治療。按照UICC(Union for International Cancer Control)2009年修訂的pTNM分期標準:Ⅰ期47例,Ⅱ期30例,Ⅲ期39例。按照WHO肺癌分類標準:鱗癌62例,腺癌39例,腺鱗癌15例。高、中分化86例,低分化30例。有淋巴結轉移59例,無淋巴結轉移57例。另收集同一患者的距癌組織>5 cm、經HE染色證實無癌細胞浸潤的正常余肺組織116例(正常組)。隨訪日期從2008年2月1日—2013年1月31日,生存期的計算從手術日期到隨訪截止日期,或由于復發、轉移而死亡的日期為止。所有標本的使用均經天津市胸科醫院倫理委員會同意,取得患者或家屬的知情。
1.2 材料和試劑 兔抗人RhoB抗體、兔抗人E-cadherin抗體均購自北京博奧森生物技術有限公司,快捷型酶標羊抗鼠/兔IgG聚合物及二氨基聯苯胺(DAB)顯色試劑盒購自福州邁新生物技術開發有限公司。
1.3 方法 手術切除后標本迅速經10%中性福爾馬林固定,常規石蠟包埋后連續切片,厚度5 μm,采用常規免疫組化Super Pic TureTMPolymer二步法檢測,嚴格按照說明書進行操作,抗原修復采用高壓高溫熱修復。采用已知陽性切片作為陽性對照,PBS代替一抗作為陰性對照。
1.4 陽性結果判斷 RhoB蛋白主要表達于細胞的膜結構上;E-cadherin陽性表達主要位于細胞膜,部分位于細胞質。根據染色細胞百分率和染色程度進行評定和分析:每例均隨機觀察10個高倍視野(×400),每個視野計數100個細胞,陽性細胞率=陽性細胞數/觀察細胞數×100%。陽性細胞率計分標準:≤10%為0分,11%~25%為1分,26%~50%為2分,51%~75%為3分,>75%為4分。染色強度:黃色為1分,棕黃色為2分,棕褐色為3分。將陽性細胞率得分和染色強度得分相乘即為最后得分:0分為陰性(-),1~4分為弱陽性(+),5~8分為中度陽性(++),9~12分為強陽性(+++)。在分析時將(-)和(+)定為低表達,(++)和(+++)定為高表達。
1.5 統計學方法 采用SPSS 17.0軟件進行數據處理,計數資料組間比較采用χ2檢驗,相關性分析用Spearman等級相關,對生存數據采用Kaplan-Meier分析并繪制生存曲線,應用Log-rank檢驗差異性,采用COX風險模型進行預后因素分析,P<0.05為差異有統計學意義。
2 結果
2.1 2組RhoB和E-cadherin的陽性表達情況比較 NSCLC組RhoB、E-cadherin陽性表達率均低于正常組(均P<0.01),見表1。2組RhoB主要表達于膜結構上(細胞膜或核膜),E-cadherin表達于細胞膜,正常組RhoB和E-cadherin的陽性表達均為高表達,見圖1~6。

Table 1 Comparison of positive expressions of RhoB and E-cadherin between two groups表1 2組RhoB、E-cadherin的陽性表達情況 例(%)
2.2 NSCLC組RhoB、E-cadherin表達與患者臨床病理特征的關系 RhoB、E-cadherin的表達強度在不同性別、年齡、吸煙與否、腫瘤部位、腫瘤最大直徑間差異均無統計學意義。不同腫瘤病理類型、腫瘤分化程度及淋巴結轉移情況下,RhoB在NSCLC組織中的表達強度差異有統計學意義;不同腫瘤分化程度、TNM分期及淋巴結轉移情況下,E-cadherin在NSCLC組織中的表達強度差異有統計學意義,見表2。
2.3 NSCLC組RhoB與E-cadherin表達的相關性分析 NSCLC組RhoB與E-cadherin的表達呈正相關(r=0.503,P<0.01),見表3。
2.4 RhoB、E-cadherin的表達與NSCLC患者預后的關系 116例NSCLC患者隨訪1~60個月,中位數44個月,失訪3例。RhoB高表達和低表達患者3年生存率分別為83.93%(47/56)和40.00%(24/60),差異有統計學意義(Log-rank χ2=18.992,P<0.01),見圖7。E-cadherin高表達和低表達患者3年生存率分別為85.11%(40/47)和44.93%(31/69),差異有統計學意義(Log-rank χ2=16.680,P<0.01),見圖8。RhoB與E-cadherin共同高表達及共同低表達者的3年生存率分別為89.19%(33/37)、34%(17/50),差異有統計學意義(Log-rank χ2=24.385,P<0.01),見圖9。
2.5 多因素COX回歸模型分析 以性別(男=1,女= 2)、年齡、病理類型、腫瘤分化程度、腫瘤最大直徑、是否有淋巴結轉移(是=1,否=2)及RhoB、E-cadherin是否共同低表達(是=1,否=2)為自變量,以生存時間為因變量,應用COX比例風險回歸模型進行分析。結果顯示RhoB和E-cadherin共同低表達、淋巴結轉移是影響NSCLC患者預后的危險因素,見表4。

Table 2 Comparison of expression intensities of RhoB and E-cadherin between different clinical pathological characteristic groups of NSCLC表2 RhoB、E-cadherin的表達與NSCLC患者臨床病理特征的關系 例(%)

Table 3 The correlation of expressions of RhoB and E-cadherin in NSCLC group表3NSCLC組RhoB與E-cadherin表達的相關性分析

Figure 7 The correlation between the expression of RhoB and the survival time of patients with NSCLC圖7 RhoB的表達與NSCLC患者生存時間的關系

Figure 8 The correlation between the expression of E-cadherin and the survival time of patients with NSCLC圖8 E-cadherin的表達與NSCLC患者生存時間的關系

Figure 9 The correlation between the high expression of both RhoB and E-cadherin,the low expression of both RhoB and E-cadherin and the survival time of patients with NSCLC圖9 RhoB和E-cadherin共同高表達及共同低表達與NSCLC患者生存時間的關系
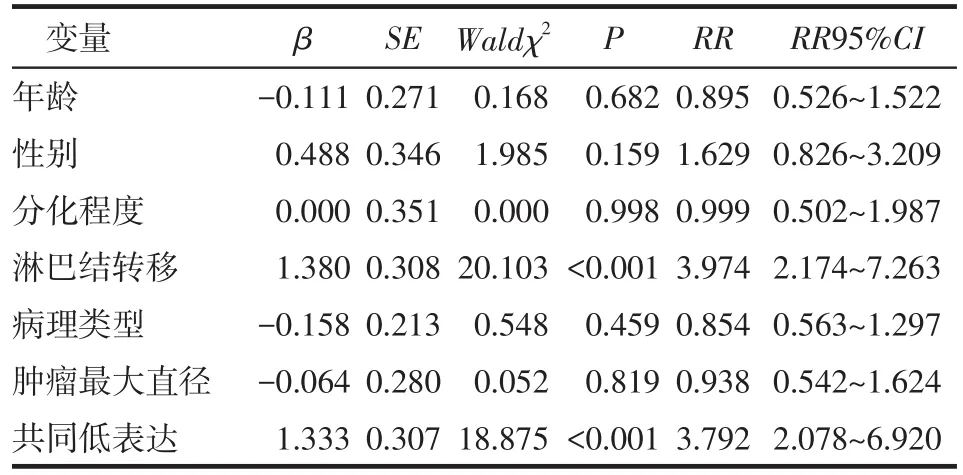
Table 4 Results of COX proportional hazards model for various prognostic factors in patients with NSCLC表4 COX比例風險回歸模型分析結果
3 討論
RhoB是Rho家族中一個較為獨特的分子,在腫瘤惡性發展過程中,RhoB的表達通常是減弱的,體外實驗也發現RhoB可抑制腫瘤細胞增殖、存活、侵襲和轉移[4]。Bousquet等[5]通過RNA干擾敲除支氣管非腫瘤細胞中的RhoB基因,發現RhoB表達降低可促進細胞遷移和侵襲。Mazieres等[6]研究發現,隨著肺癌浸潤性增高,RhoB在癌組織中的表達量大幅度下降,同時RhoB表達丟失與肺癌的高分期、高浸潤性、低分化、高增殖指數等存在顯著相關性,而RhoB過表達的A549細胞的增殖、生長等均顯著下降。Sato等[7]研究顯示112例原發NSCLC中有64例RhoB為不表達或低表達,與本研究結果一致。本研究中RhoB在正常余肺組織中呈高表達,在NSCLC組織中表達顯著降低,且其在不同腫瘤病理類型、腫瘤分化程度及淋巴結轉移情況間表達強度不同。
E-cadherin陽性表達有抑制腫瘤轉移的功能,E-cadherin表達下降或缺失,細胞黏附力下降,造成細胞容易分散而向外周浸潤性生長,一旦獲得轉移的必要條件,就可脫離原發灶而發生侵襲和轉移[3]。近年來通過在肺癌、乳腺癌、甲狀腺乳頭狀癌、膀胱癌、前列腺癌、大腸癌及鼻咽癌等腫瘤的研究中證實,E-cadherin表達降低與腫瘤的分化、侵襲和轉移有顯著相關性[8]。本研究中E-cadherin同樣在大部分NSCLC組織中表達顯著降低,其表達強度在不同TNM分期、腫瘤分化程度及淋巴結轉移間有差異。
本研究結果顯示,RhoB和E-cadherin共同高表達或共同低表達更容易出現在腺鱗癌、低分化、高分期及有淋巴結轉移的患者中,且RhoB和E-cadherin共同低表達是致使NSCLC患者預后較差的危險因素。NSCLC組織中RhoB與E-cadherin的表達具有較好的相關性和一致性,提示RhoB和E-cadherin在促進腫瘤的發生、浸潤的信號傳導通路中發揮著相似的作用。RhoB在肺癌中的低表達或不表達可能主要是由組蛋白低乙酰化所引起,在應用組蛋白去乙酰化酶抑制劑處理后的肺癌細胞系中可見顯著的RhoB低表達[9]。而RhoB低表達可促進支氣管上皮細胞的遷移和浸潤,其主要是通過激活絲/蘇氨酸蛋白激酶(Akt)并依賴于Rac1的激活,從而導致磷脂酰肌醇3-激酶(PI3K)-Akt信號通路被激活[5]。Kazerounian等[10]發現RhoB缺失可促進腫瘤的生成及腫瘤細胞的生長,促進Akt信號傳導通路在乳腺癌腫瘤細胞的發生。Howe等[11]提出RhoB在內皮細胞的遷移、出芽和毛細血管形成中發揮重要作用,其部分機制為抑制RhoA/ROCK信號通路。由此可見,RhoB表達丟失可能是肺癌細胞獲得浸潤性的特征之一,其作用機制可能和PI3K/Akt信號通路被激活有關。研究還發現,E-cadherin通過介導表皮生長因子受體對PI3K/Akt的激活而對腫瘤細胞增殖產生作用[12]。E-cadherin可抑制NSCLC細胞的增殖和浸潤,可能通過下調RhoA或Cdc42的表達來實現,當敲除RhoA或Cdc42基因,使NSCLC細胞增殖和浸潤能力均顯著下降[13]。可見,RhoB和E-cadherin在腫瘤發生發展的信號傳導通路中有一定的交叉點。

Figure 1 The expression of RhoB in squamous carcinoma圖1 RhoB在鱗癌中的表達(SP,×400)

Figure 2 The expression of RhoB in adenocarcinoma圖2 RhoB在腺癌中的表達(SP,×400)

Figure 3 The expression of E-cadherin in adenocarcinoma圖3 E-cadherin在腺癌中的表達(SP,×400)

Figure 4 The expression of E-cadherin in squamous carcinoma圖4 E-cadherin在鱗癌中的表達(SP,×400)

Figure 5 The expression of RhoB in the normal lung tissue圖5 RhoB在正常余肺中的表達(SP,×400)

Figure 6 The expression of E-cadherin in the normal lung tissue圖6 E-cadherin在正常余肺中的表達(SP,×400)
[1] 陳萬青,張思維,鄒小農.中國肺癌發病死亡的估計和流行趨勢研究[J].中國肺癌雜志,2010,13(5):283-285.
[2]Wojciak-Stothard B,Zhao L,Oliver E,et al.Role of RhoB in the regulation of pulmonary endothelial and smooth muscle cell responses to hypoxia[J].Circ Res,2012,110(11):1423-1434.
[3] Reinhold WC,Reimers MA,Lorenzi P,et al.Multifactorial regulation of E-cadherin expression:an integrative study[J].Mol Cancer Ther,2010,9(1):1-16.
[4]Alfano D,Ragno P,Stoppelli MP,et al.RhoB regulates uPAR signalling[J].J Cell Sci,2012,125(Pt 10):2369-2380.
[5]Bousquet E,Mazières J,Privat M,et al.Loss of RhoB expression promotes migration and invasion of human bronchial cells via activation of AKT1[J].Cancer Res,2009,69(15):6092-6099.
[6] Mazieres J,Antonia T,Daste G,et al.Loss of RhoB expression in human lung cancer progression[J].Clin Cancer Res,2004,10(8): 2742-2750.
[7]Sato N,Fukui T,Taniguchi T,et al.RhoB is frequently downregulated in non-small-cell lung cancer and resides in the 2p24 homozygous deletion region of a lung cancer cell line[J].Int J Cancer, 2007,120(3):543-551.
[8]Yap AS,Crampon MS,Hardin J.Making and breaking contacts:the cellular biology of cadherin regulation[J].Curr Opin Cell Biol, 2007,19(5):508-514.
[9] Mazières J,Tovar D,He B,et al.Epigenetic regulation of RhoB loss of expression in lung cancer[J].BMC Cancer,2007,7:220.
[10]Kazerounian S,Gerald D,Huang M,et al.RhoB differentially controls Akt function in tumor cells and stromal endothelial cells during breast tumorigenesis[J].Cancer Res,2013,73(1):50-61.
[11]Howe GA,Addison CL.RhoB controls endothelial cell morphogenesis in part via negative regulation of RhoA[J].Vasc Cell,2012,4:1.
[12]劉聯,張昕,王秀問,等.E-鈣粘素介導的細胞粘附通過EGFR激活卵巢癌細胞P13K-Akt信號通路[J].現代婦產科進展,2007,16 (4):270-273.
[13]Asnaghi L,Vass WC,Quadri R,et al.E-cadherin negatively regulates neoplastic growth in non-small cell lung cancer:role of Rho GTPases[J].Oncogene,2010,29(19):2760-2771.
(2013-06-01收稿 2013-08-01修回)
(本文編輯 陳麗潔)
The Expression and Clinical Significance of RhoB and E-Cadherin in Non-Small-Cell Lung Cancer Tissues
TAN Yimei1,ZHANG Xun2,XU Meilin3,WANG Jing3,XU Yijun2
1 Tianjin Medical University,Tianjin 300070,China;2 Department of Thoracic Surgery,3 Department of Pathology,Tianjin Chest Hospital
ObjectiveTo investigate the expressions of RhoB and E-cadherin in non-small-cell lung cancer (NSCLC),and their clinical significances thereof.MethodsImmunohistochemical staining was applied to detect expressions of RhoB and E-cadherin in 116 samples of NSCLC(NSCLC group)and 116 samples of normal lung tissues(control group).Correlations of expressions of RhoB and E-cadherin to clinical pathological parameters and prognosis were analyzed in two groups.ResultsThe expression intensities of RhoB and E-cadherin were significantly lower in NSCLC group than those in control group(57.76%vs 87.07%,54.31%vs 85.34%,P<0.01).There were significant differences in the expression of RhoB between different pathological types,differentiation and lymph node metastasis in NSCLC group.There were significant differences in the expression of E-cadherin between different TNM stages,differentiation and lymph node metastasis in NSCLC group.The expression of RhoB was positively correlated with the expression of E-cadherin(r=0.503,P<0.01).The 3-year survival rates were significantly higher in patients with high expression of RhoB(83.93%)than those in patients with low expression of RhoB(40.00%,Log-rank χ2=18.992,P<0.01).The 3-year survival rates were significantly higher in patients with high expression of E-cadherin(85.11%)than those in patients with low expression of E-cadherin (44.93%,Log-rank χ2=16.680,P<0.01).Further multivariate analysis suggested that both lower expressions of RhoB and E-cadherin and lymph node metastasis were prognostic indicators for NSCLC(P<0.001).ConclusionThe expressions of RhoB and E-cadherin showed a good correlation in NSCLC.Detecting the expression of RhoB combined with E-cadherin may give a clue on clinicopathological features and prognosis in patients with NSCLC.
carcinoma,non-small-cell lung cancer;cadherins;immunohistochemistry;prognosis;Kaplan-Meiers estimate;RhoB;E-cadherin
R734.2
A【DOI】10.3969/j.issn.0253-9896.2014.01.009
1天津醫科大學(郵編300070);2天津市胸科醫院胸外科,3病理科
△通訊作者 E-mail:zhangxun69@163.com
猜你喜歡
保健醫苑(2023年2期)2023-03-15 09:03:04
音樂探索(2022年2期)2022-05-30 21:01:37
中國臨床醫學影像雜志(2022年2期)2022-05-25 13:24:34
小天使·一年級語數英綜合(2019年8期)2019-08-27 02:23:00
中國特種設備安全(2018年11期)2019-01-08 02:08:32
小學科學(學生版)(2018年7期)2018-08-13 09:33:04
癌變·畸變·突變(2016年3期)2016-02-27 06:15:34
醫學研究雜志(2015年12期)2015-06-10 06:57:46
鄭州大學學報(醫學版)(2015年2期)2015-02-27 14:50:46
鄭州大學學報(醫學版)(2015年1期)2015-02-27 14:50:26
