肝硬化門靜脈高壓性外周血細胞減少對手術預后的影響
2015-04-14 09:30:23呂云福宮曉光韓曉玉常順伍黎業娟
海南醫學 2015年13期
關鍵詞:手術
呂云福,宮曉光,韓曉玉,常順伍,黎業娟,鄧 杰
(海南省人民醫院普通外科,海南 海口 570311)
肝硬化門靜脈高壓性外周血細胞減少對手術預后的影響
呂云福,宮曉光,韓曉玉,常順伍,黎業娟,鄧 杰
(海南省人民醫院普通外科,海南 海口 570311)
目的 探討外周血細胞減少對手術預后的影晌,并從外周血細胞減少的角度提出治療策略。方法回顧性分析1991年1月至2011年6月海南省人民醫院普通外科收治的366例肝炎后肝硬化門靜脈高壓性脾腫大患者的臨床資料。結果三種血細胞計數均正常者36例(9.8%),并發一種以上外周血細胞減少者330例,其中單種血細胞減少占30.0%(99/330),兩種血細胞減少占35.8%(118/330),三種血細胞均減少占34.2%(113/330)。全組均行脾臟切除+門奇斷流術或分流術。血細胞正常組與血細胞減少組手術預后比較差異有統計學意義(P<0.05)。單種血細胞減少與多種血細胞減少的手術預后比較差異也有統計學意義(P<0.05)。在白細胞(WBC)、紅細胞(RBC)和血小板(PLT)減少的三個因素中,僅PLT減少對手術預后有明顯影響,差異有統計學意義(P<0.05)。結論外周血細胞減少對手術預后有一定影響,單種血細胞減少的手術預后明顯優于多種血細胞減少,血細胞減少越多越重、預后越差,PLT減少是影響手術預后的主要因素,重度PLT減少應切除腫大的脾臟。
肝硬化門靜脈高壓癥;外周血細胞減少;手術預后;影響
肝炎后肝硬化門靜脈高壓性脾腫大病人并發嚴重消化道出血,嚴重脾亢和肝癌時,通常需要手術治療,影響手術預后的因素盡管有多種[1],但外周血細胞減少是一種不可忽視的因素。外周血細胞減少是指外周靜脈血中抽出的血液中細胞計數低于正常檢測值,即白細胞(WBC<4.0×109/L),紅細胞(RBC<3.5×1012/L)和血小板(PLT<100×109/L)。本文回顧性分析1991年1月至2011年12月海南省人民醫院普外科收治的366例肝炎后肝硬化門靜脈高壓性脾腫大患者的臨床資料,探討外周血細胞減少對手術預后的影響,現報道如下:
1 資料與方法
1.1 一般資料 366例患者中男性250例,女性116例,男女之比為2.2:1,年齡5~79歲,平均43歲。所有患者均為肝炎后肝硬化,并在術中取肝組織經病理檢查證實脾臟普遍增大,B超或CT測量脾臟大小平均為224 mm×159 mm×95 mm。上消化道造影或胃鏡檢查均顯示食管下段和胃底均有中、重度靜脈曲張。74例(20.2%)因消化道出血而入院,248例(67.8%)既往有出血史。所有患者均經輸血,補充已缺少的血液有形成分后行脾切除術,同時行賁門周圍血管離斷術356例(附加脾腎靜脈分流56例),行腸腔靜脈分流術和門腔靜脈分流術各5例。
1.2 方法 先設計表格,然后按表格的內容如年齡、性別、住院號、入院診斷、出院診斷、三系血細胞計數、治療方法、術后并發癥、治療結果等26項內容和收治年月的先后順序逐例逐項地進行登記統計、分析,項目內容不全者未列入本研究范圍。手術預后主要由痊愈、好轉和死亡三種狀況組成。痊愈是指腹水、腹脹及出血癥狀消失,減少的血細胞開始上升并接近正常值,肝臟功能改善,術后無嚴重并發癥,能安全出院;死亡是指術后住院期間死亡、包括病情危重,患者家屬要求出院后1周內的死亡;否則為好轉。單種血細胞減少是指血液3系血細胞中只有某一種血細胞減少,多種血細胞減少是指兩種以上血細胞減少。
1.3 統計學方法 應用SPSS19.0統計軟件,計數資料比較采用χ2檢驗,多單因素分析采用多元線性回歸處理,以P<0.05表示差異有統計學意義。
2 結果
2.1 血細胞計數情況 366例患者中三種血細胞計數均正常者36例(9.8%),并發一種以上外周血細胞減少者330例(90.2%),其中單種血細胞減少占30.0%(99/330),兩種血細胞減少占35.8%(118/330),三種血細胞計數均減少占34.2%(113/330)。
2.2 血細胞正常組與減少組患者的手術預后比較 血細胞正常組與血細胞減少組手術預后比較差異有統計學意義(χ2=6.222,P<0.05),見表1。

表1 血細胞正常組與減少組患者的手術預后比較[例(%)]
2.3 單種血細胞減少與多種血細胞減少療效比較 單種血細胞減少與多種血細胞減少的手術預后比較差異也有統計學意義(χ2=7.819,P<0.05),見表2。

表2 單種血細胞減少與多種血細胞減少療效比較[例(%)]
2.4 三系血細胞的多元線性回歸分析 在WBC、RBC和PLT減少的三個因素中比較,僅PLT有差異有統計學意義(P<0.05),提示PLT減少是影響手術預后的主要因素,見表3。
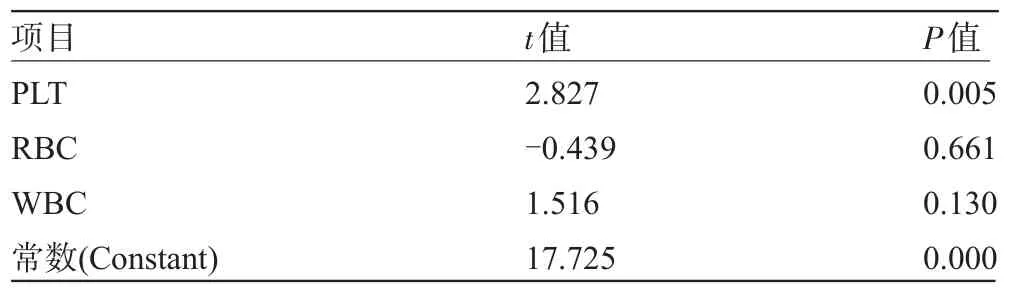
表3 三系血細胞的多元線性回歸分析
3 討論
肝硬化門靜脈高壓性脾臟腫大90%患者并發血細胞減少,其中70%表現為多種血細胞減少,30%表現為單種血細胞減少[2]。
外周血細胞減少對預后的影響,以往只是停留在人們的印象中,沒有研究證據。本研究大數據資料表明,血細胞正常組的手術預后明顯優于血細胞減少組(P<0.05)。無論是單種血細胞減少還是多種血細胞減少,它們的手術預后都比血細胞正常組明顯差。
單種血細胞減少的術后療效明顯優于多種血細胞減少(P<0.05),血細胞減少的種類越多越嚴重預后越差。它不僅與脾功能亢進有關[3],而且還與肝炎病毒感染及骨髓的代償調節有關[4]。要提高手術的安全性,術前應加強保肝,改善肝臟功能,應用提升血細胞的藥物,給予成份輸血或輸全血,將減少的血細胞提升到正常或接近至正常水平,手術才比較安全。門靜脈高壓性靜脈曲張破裂出血是威協生命的并發癥[5]。近年來,對門靜脈高壓性上消化道出血患者多選擇創傷較小的內鏡血管栓塞術或套扎術[6-7]和TIPS支架治療[8-10],但TIPS手術不能改善PLT減少[11],當非手術治療無效時才考慮手術,即使需要開腹手術,也以遠端脾腎分流術為首選,不推薦做破壞門靜脈完整性大、腦病發生率高的門-腔分流術[12]。本組病例均行脾切除術,盡管當時對于出于消化道出血、巨脾或脾功能亢進等多種原因考慮,但從現代觀點來看,手術適應證是放寬了。然而,本研究的結果和結論對未來治療方案的選擇,特別是對需要手術的病例、如何做好圍手術期處理和判斷預后還是很有參考價值的。肝硬化門靜脈高壓性脾腫大病人的手術預后與血細胞是否減少和減少的程度有關。血細胞減少越嚴重手術預后越差。
本文研究資料顯示PLT減少是影響手術預后的主要因素。60%肝硬化門靜脈高壓性脾腫大患者存在PLT減少[13],PLT計數<50×109/L時均伴有兩種以上的血細胞減少,其中伴有3種血細胞減少占77%,PLT計數<30×109/L時伴有3種血細胞減少占85%,兩者比較差異有統計學意義(χ2=5.138,P=0.025)。PLT計數>50×109/L時宜選非手術治療,尤其血細胞正常的病例盡管它存在上消化道出血或脾腫大等因素也應該選擇非手術;PLT計數50×109/L至30×109/L時原則上也主張非手術,病情不能控制時才考慮手術治療;PLT計數<30×109/L時宜選手術治療。PLT減少常常伴有纖維蛋白原減低,纖維蛋白原是一種與凝血有關的蛋白質,嚴重減低也會增加出血傾向[14],術前輸冷沉淀、將纖維蛋白原補充至正常水平可能效果更好[15]。手術宜小不宜大,僅切除脾臟,附加斷流術或脾腎分流術即可,切忌手術時間過長,否則會帶來不良后果。巨脾切除后大多數患者PLT計數會明顯增加[16]。
[1]楊 鎮,裘法祖.關于門靜脈高壓癥預后結局的研究[J].腹部外科,2003,16(2):68-70.
[2]呂云福,李新秋,黃偉煒,等.門靜脈高壓性脾功能亢進患者的外周血細胞變化[J].中華普通外科雜志,2007,22(9):702.
[3]閆 峰,李 威,陳君填,等.基因芯片篩選門靜脈高壓癥脾亢脾和正常脾巨噬細胞中差異表達基因[J].南方醫科大學學報,26(11): 1548-1551.
[4]Lv YF,Li XQ,Xie XH,et al.Portal hypertension splenomegaly is not always associated with hematocytopenia[J].Journal of US-China Medical Science,2009,6(1):28-30.
[5]O'Brien J,Triantos C,Burroughs AK.Management of varices in patients with cirrhosis[J].Nat Rev Gastroenterol Hepatol,2013,10 (7):402-412.
[6]Bandika VL,Goddard EA,De Lacey RD,et al.Endoscopic injection sclerotherapy for bleeding varices in children with intrahepatic and extrahepatic portal venous obstruction:benefit of injection tract embolisation[J].SAfr Med J,2012,102(11 Pt 2):884-887.
[7]Kim DO,Ul'ianov DN,Vasnev OS.Endoscopic treatment of gastric varicesbleeding[J].Eksp Klin Gastroenterol,2012,(6):58-61.
[8]Garcia-Tsao G,Sanyal AJ,Grace ND,et al.Prevention and management of gastroesophagealvarices and variceal hemorrhage in cirrhosis[J].Hepatology,2007,46(3):922-938.
[9]García-Pagán JC,Caca K,Bureau C,et al.Early use of TIPS in patients with cirrhosis and variceal bleeding[J].N Engl J Med,2010, 362(25):2370-2379.
[10]de Franchis R,Baveno V Faculty.Revising consensus in portal hypertension:Report of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension[J].J Hepatol,2010,53(4):762-768.
[11]Barney EJ,Little EC,Gerkin RD,et al.Coatedtransjugular intrahepatic portosystemic shunt does not improve thrombocytopenia in patients with liver cirrhosis[J].Dig Dis Sci,2012,57(9):2430-2437.
[12]冷希圣.門靜脈高壓癥與新斷流手術.第16屆全國普通外科學術會議暨第十二屆全國門靜脈高壓癥學術研討會論文匯編,2012: 20-25.
[13]Karasu Z,Gurakar A,Kerwin B,et al.Effect of transjuqular intrahepatic portosystemic shunt on thrombocytopenia associated with cirrhosis[J].Dig Dis Sci,2001,46(2):449-456.
[14]Platè M,Asselta R,Spena S,et al.Congenitalhypofibrinogenemia: characterization of two missense mutations affecting fibrinogen assembly and secretion[J].Blood Cells Mol Dis,2008,41(3): 292-297.
[15]Cui Y,Hei F,Long C,et al.Perioperative monitoring of thromboelastograph On hemostasis and therapy for cyanotic infants undergoing complex cardiac surgery[J].Artif Organs,2009,33(11):909-14.
[16]Lu YF,Li XQ,Han XY,et al.Peripheralblood cell variations in cirrhotic portal hypertension patients with hypersplenism[J].Asian Pac J Trop Med,2013,6(8):663-666.
Effect of peripheral cytopenias due to cirrhotic portal hypertension on postoperative prognosis.
LV Yun-fu, GONG Xiao-guang,HAN Xiao-yu,CHANG Shun-wu,LI Ye-juan,DENG Jie.
Department of General Surgery,People's Hospital of Hainan Province,Haikou 570311,Hainan,CHINA
ObjectiveTo investigate the effect of peripheral cytopenias on the operative prognosis in patients with cirrhotic portal hypertension,so as to put forward the treatment strategies from the perspective of peripheral cytopenias.MethodsA retrospective analysis was performed on the clinical data of 366 patients with splenomegaly of posthepatitic cirrhotic portal hypertension in Department of General Surgery,People's Hospital of Hainan Province from January 1991 to June 2011.All data were processed with SPSS19.0,and the χ2test was used for univariate analysis.Comparisons between thrombocytopenia,leucopenia,and erythropenia were conducted by multiple linear regression analysis.ResultsThirty-six patients(9.8%)had a normal blood cell count and 330 patients had peripheral cytopenias,in which mono-lineage cytopenias accounted for 30.0%(99/330),bi-lineage cytopenias accounted for 35.8%(118/330),and tri-lineage cytopenias accounted for 34.2%(113/330).There were significant statistical differences in the postoperative prognosis between the normal blood and the cytopenias(P<0.05),as well as between mono-lineage cytopenias and multi-linage cytopenias(P<0.05).In comparison,among leucopenia,erythropenia and thrombocytopenia,only thrombocytopenia showed a significant influence on the postoperative prognosis(P<0.05).ConclusionPeripheral cytopenias can exert definite influences on postoperative prognosis.Patients with mono-lineage cytopenias have significantly better surgical outcomes than those with multi-lineage cytopenias.The more severe the cytopenias,the poorer the surgical outcome.Thrombocytopenia is the major influencing factor of surgical outcome,and splenectomy could be an effective treatment for splenomegaly associated with severe thrombocytopenia.
Cirrhotic portal hypertension;Peripheral cytopenias;Postoperative prognosis;Effect
R657.3+1
A
1003—6350(2015)13—1906—03
10.3969/j.issn.1003-6350.2015.13.0687
2015-05-05)
海南省重點科技計劃項目(編號:ZDXM2014068)
呂云福。E-mail:yunfu_lv@126.com
猜你喜歡
環球時報(2022-12-23)2022-12-23 09:28:37
昆明醫科大學學報(2022年1期)2022-02-28 07:45:04
中老年保健(2021年11期)2021-08-22 03:13:36
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
河北畫報(2020年10期)2020-11-26 07:20:50
小學閱讀指南·低年級版(2017年1期)2017-03-13 20:07:35
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
中國醫療美容(2015年1期)2015-07-12 10:06:38
鄭州大學學報(醫學版)(2015年2期)2015-02-27 14:50:54
西南軍醫(2014年5期)2014-04-25 07:42:48