血糖增高對急性心肌梗死患者的預后影響
2017-04-27 23:16:02湯長春陳然李祥賈穎黃玉艷
中國現代醫生 2017年7期
湯長春+陳然+李祥+賈穎+黃玉艷

[摘要] 目的 探討血糖增高對急性心肌梗死(AMI)患者住院期間及遠期影響。 方法 入選AMI患者895例,按入院時血糖高低分兩組,其中高血糖組(425例),正常血糖組(470例),比較兩組患者的遠期觀察影響。 結果 兩組AMI患者住院期間死亡率比較,無明顯差異(P>0.05),但高血糖組在心衰發生率及惡性心律失常事件發生率明顯上升,差異有統計學意義(P<0.05)。患者出院后1年隨訪,兩組患者死亡率比較,差異無統計學意義(P>0.05),但正常血糖組在再住院率、糖尿病發生率、心衰發生率及惡性心律失常事件發生率較高血糖組明顯下降,差異有統計學意義(P<0.05)。結論 血糖增高可能會導致AMI患者心衰及再住院率增加,并轉化糖尿病增多。
[關鍵詞] 高血糖;急性心肌梗死;遠期影響;并發癥
[中圖分類號] R542.2+2 [文獻標識碼] B [文章編號] 1673-9701(2017)07-0037-03
[Abstract] Objective To investigate the effects of increased blood glucose on acute myocardial infarction (AMI) patients during hospitalization and for a long term. Methods A total of 895 patients with AMI were enrolled and divided into two groups including high blood glucose group (n=425) and normal blood glucose group (n=470),according to the level of blood glucose at admission. The effects of long-term observation were compared between the two groups. Results There was no significant difference in mortality rate between the two groups during hospitalization of AMI(P>0.05). While the incidences of heart failure and malignant arrhythmia in the hyperglycemia group were significantly higher than those in the control group ,and the differences were statistically significant(P<0.05). There were no significant difference in mortality rate between the two groups within 1 year follow-up after discharge(P>0.05).However, the incidences of rehospitalization, diabetes mellitus, heart failure and malignant arrhythmia in the normal blood glucose group were significantly lower than those of the hyperglycemia group(P<0.05), and the differences were statistically significant (P<0.05). Conclusion Elevated blood glucose may cause the patients with AMI increase of heart failure, rehospitalization rate and the conversion of diabetes.
[Key words] Hyperglycemia;Acute myocardial infarction;Long-term effects;Complications
患者發生急性心肌梗死(acute myocardial infarction,AMI)時常伴有血糖增高現象,大多情況下考慮為急性應激所致,目前國外有報道在AMI后非糖尿病患者大約有25%~50%發生應激性高血糖,那么,AMI合并高血糖患者在住院期間及遠期預后有怎樣的聯系,值得我們進一步研究。本文隨訪研究血糖增高對AMI患者預后影響,現報道如下。
1 對象和方法
1.1 研究對象
回顧性分析2013年6月~2015年5月在我院治療的 895 例 AMI 患者,男 450 例,女 445 例,平均(66.1±24)歲,將血糖結果分為正常血糖組(470 例)和高血糖組(425 例),正常血糖組:入院隨機血糖<7.8 mmol/L,且入院第2天空腹血糖<6.1 mmol/L;高血糖組:入院隨機血糖≥11.1 mmol/L,或(和)入院第2天空腹血糖≥6.1 mmol/L。入院隨機血糖在 7.8~11.1 mmol/L 之間不納入本研究,診斷標準符合美國心臟病協會和美國心臟病學會診療指南 [1],包括急性非 ST 段上抬心肌梗死和急性 ST 段上抬心肌梗死,但有手術史、創傷史、肺源性心臟病、先天性心臟病、嚴重肝腎功能不全者、惡性腫瘤及既往已知明確糖尿病史者均排除。兩組患者住院期間一般資料比較,差異無統計學意義(P>0.05),具有可比性。見表1。
1.2 方法
入院后即靜脈采血2 mL,以酶法測定血糖,根據血糖結果分為高血糖組和血糖正常組,住院期間登記兩組患者的一般情況,如年齡、性別、合并高血壓病、有無吸煙及血糖血脂情況,觀察住院期間死亡率、心衰發生率及惡性心律失常事件發生率,出院后1年隨訪患者,并行動態心電圖、肝腎功能等常規生化檢查,了解兩組患者死亡率、再住院率、糖尿病發生率、心衰發生率及惡性心律失常事件發生率。嚴重心律失常事件包括頻發室性早搏、持續性或短陣室性心動過速、二度以上房室傳導阻滯、心室顫動或心室撲動,以動態心電圖檢查結果為準。糖尿病發生率是指患者隨訪1年后來院常規行 OTGG 試驗兩次為陽性時方可確診。
1.3 統計學方法
采用SPSS 17.0軟件進行統計學分析,計數資料以[n(%)]表示,采用χ2檢驗;計量資料以(x±s)表示,采用兩樣本均數比較的t檢驗,P<0.05表示差異有統計學意義。
2 結果
2.1 兩組患者住院期間死亡率及并發癥比較
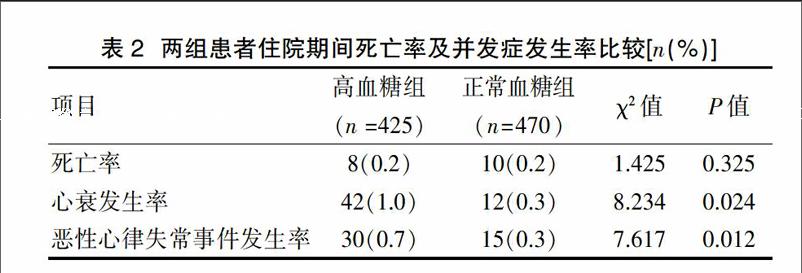
住院期間兩組患者死亡率比較,差異無統計學意義(P>0.05),但心衰及惡性心律失常事件發生率比較,高血糖組明顯上升,差異有統計學意義(P<0.05)。見表2。
2.2 出院后1年隨訪患者各參數比較
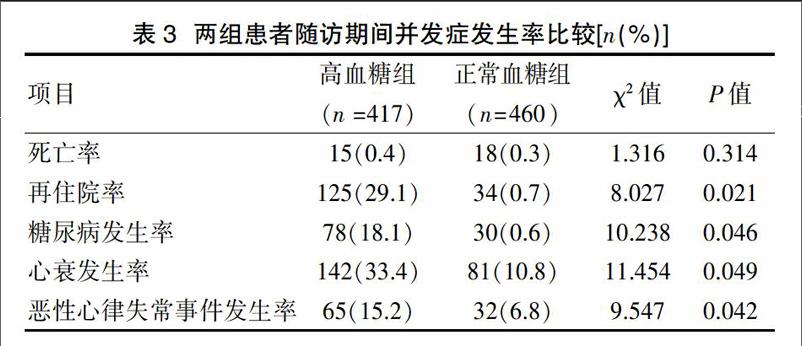
患者出院后1年隨訪,行動態心電圖、肝腎功能等常規生化檢查,并比較兩組患者死亡率、再住院率、糖尿病發生率,心衰發生率及惡性心律失常事件發生率,發現在死亡率兩組患者比較,差異無統計學意義(P>0.05),但正常血糖組在再住院率、糖尿病發生率,心衰發生率及惡性心律失常事件發生率較高血糖組顯著下降,差異有統計學意義(P<0.05)。見表3。
3 討論
急性心肌梗死患者合并高血糖在臨床患者中常見,是 AMI 患者出現應激反應的一種表現,其他觀察資料提示高血糖可能導致重要器官功能衰竭,有嚴重危及患者生命的可能[2],在本研究中發現高血糖組患者住院期間,在發生惡性心律失常、心衰發生率方面顯著高于正常血糖組,說明高血糖可影響 AMI 的心肌灌注[3],加重心肌再灌注損傷,導致心肌損害加速惡化,增加心血管事件發生,導致心肌梗死患者的死亡率增加。血糖增高考慮與 AMI 時出現應激有關[4],因為 AMI 時容易出現自主神經、內分泌功能紊亂,且出血高血糖時會加重心肌細胞代謝障礙及胰島素抵抗和高胰島素血癥[5],更加容易加重心肌損傷,并導致人胰島素相對或絕對不足,血漿游離脂肪酸濃度偏高,同時脂肪酸增高導致使損傷的心肌耗氧量更加增高,使心肌收縮力明顯減弱,增加 β 受體興奮性,從而導致心肌細胞膜受損,使細胞膜內外鈣離子平衡失常,容易引起心律失常[6]。
在隨訪期間,發現高血糖組患者在再住院率、心衰發生率及惡性心律失常事件發生率均高于正常血糖組患者,說明從長期看,高血糖組患者嚴重影響心肌梗死患者的預后,這是因為高血糖會導致血管滲透壓壓差增高[7],導致細胞內脫水,更容易造成血管內皮細胞增生或變性,從而導致血管血液動力學內穩態平衡打破,當然也容易造成外周血管收縮強烈,同時心肌細胞也會引起收縮[8],從而造成心肌梗死患者心功能出現嚴重下降,最終增加死亡率,也容易加速惡性心律失常的發生,極大的影響患者生存預后,這與劉君等[9]研究的結果大致相同。國外的資料顯示應激性高血糖是心血管事件發生的危險因素,增加了死亡率[10],AMI是冠心病的最危險階段之一,資料也提示高血糖對該心肌梗死患者并發癥發生提示統計學差異[11],其他報道也指出合并應激性高血糖的心血管事件發生率是未合并應激性高血糖的2 倍,觀察組心血管事件發生率36.11%,對照組心血管事件發生率13.33%,觀察組是對照組的2.7 倍[12],該研究基本跟本文報道的大致相同,說明高血糖對AMI患者的心肌生理功能有嚴重影響。
高血糖組患者在出院后轉化糖尿病患者比例較正常血糖組明顯增加,說明可能高血糖組患者存在胰島素的相對不足[13],隨訪發現這與患者飲食結構未調整及運動幅度未達標等也有關聯[14],潛在表明患者有轉化糖尿病趨勢,此時應重點干預患者飲食結構,控制好血糖,減少或延緩糖尿病的發生[15],因此,對此類高血糖的 AMI 患者,應重點加強宣教糖尿病知識,防范糖尿病的發生,更好提高患者生活質量。
綜上所述,對于臨床上有高血糖心肌梗死患者應特別重視,應長期宣教,控制好飲食,加強血糖監測,積極干預,防范向糖尿病轉化,從而降低心肌梗死的病死率,減少再住院率。
[參考文獻]
[1] Thygesen K,Alpert JS,Jaffe AS,et al.Third universal definition of myocardial infarction[J].Eur Heart,2012,33(20):2551-2267.
[2] Bissinger A,Grycewicz T,Grabowicz W,et al. Endothelial function and left ventricular remodeling in diabetic and non-diabetic patients after acutecoronary syndrome[J].Med Sci Monit,.2011,17(2): 73-77.
[3] Rajesh Vedanthan,Benjamin Seligman,Valentin Fuster.Global Perspective on Acute Coronary syndrome:A burden on the young and poor[J].Circulation Research,2014,114(12): 1959-1975.
[4] Won KB,Hur SH,Cho YK,et al.Comparison of 2-year mortality according to obesity in stabilized patients with type 2 diabetes mellitus after acute myocardial infarction:Results from the diamond prospective cohort registry[J].Cardiovasc Diabetol,2015,14(1):141-143.
[5] Ishida K,Geshi T,Nakano A,et al. Beneficial effects of statin treatment on coronary microvascular dysfunction and left ventricular remodeling in patients with acute myocardial infarction[J].Int J Cardiol,2012,155(3):442-447.
[6] Shroff GR,Li S,Herzog CA.Trends in mortality following acute myocardial infarction among dialysis patients in the United States over 15 years[J].Am Heart Assoc,2015,4:(10)465-468
[7] Katz P,Leiter LA,Mellbin L,et al. The clinical burden of type 2 diabetes in patients with acute coronary syndromes:Prognosis and implications for short and long term management[J].Diab Vasc Dis Res,2014,11(6):395.
[8] Han JH,Lindsell CJ,Storrow AB,et al. The Role of cardiac risk factor burden in diagnosing acute coronary syndromes in the emergency separtment setting[J].Annals of Emergency Medicine,2007,49(2):145.
[9] 劉君,萬云高,王慧娟,等.糖尿病對急性心肌梗死患者近期預后的影響分析[J].中華老年心腦血管病雜志. 2012,14(2): 146-148
[10] Armas NB, Ortega YY, Suárez R, et al. Early acute myocardia infarction mortality in cuba[J].MEDICC Rev, 2012,14(4): 19-25
[11] 湯長春,陳然,劉趙云,等.急性心肌梗死患者血糖增高對住院期間預后影響[J].中華老年心腦血管病雜志,2016,18(2):158-160
[12] Cheung NW,Weng VW,Mclean M.The hyperglycemia intensive insulin infusion in infarction(HL-5)study:A randomized controlled trial of in sulin infusion therapy for myocardial infarction[J].Diabetes Care,2014,29(4):765-770.
[13] Tetsuya Tanaka,Shinji Seto,Kazuto Yamamoto,et al. An assessment of risk factors for the complexity of coronary artery disease using the syntax score[J].Cardiovascular Intervention and Therapeutics,2013,9(2):75-77.
[14] Sebastian Reith,Simone Battermann,Martin Hellmich,et al. Impact of type 2 diabetes mellitus and glucose control on fractional flow reserve measurements in intermediate grade coronary lesions[J].Clinical Research in Cardiology,2014,18:(3)191-201.
[15] McArdle MA,Fonucane OM,Connaughton RM,et al. Mechaisms of obesity-induced inflammation and insulin and insulin resietance:Insights into emerging role nutritional atrategies[J].Front Endocrinol (Lausanne),2013,10(3):11-14.
(收稿日期:2016-12-11)
猜你喜歡
今日健康(2016年12期)2016-11-17 19:24:29
今日健康(2016年12期)2016-11-17 13:16:30
今日健康(2016年12期)2016-11-17 13:09:54
今日健康(2016年12期)2016-11-17 12:06:09
人間(2016年27期)2016-11-11 17:32:04
人人健康(2016年21期)2016-11-05 11:32:22
科技視界(2016年18期)2016-11-03 21:58:33
中國實用醫藥(2016年24期)2016-10-17 05:58:58
中國實用醫藥(2016年24期)2016-10-17 05:31:56
中國實用醫藥(2016年24期)2016-10-17 04:11:14