白內障患者術后聯用激素和非甾體抗炎藥的臨床效果考察
2017-05-02 09:28:04劉暉劉剛羅莉麗
當代醫學 2017年11期
關鍵詞:差異
劉暉,劉剛,羅莉麗
(四川省內江市第一人民醫院眼科,四川 內江 641000)
白內障患者術后聯用激素和非甾體抗炎藥的臨床效果考察
劉暉,劉剛,羅莉麗
(四川省內江市第一人民醫院眼科,四川 內江 641000)
目的 研究白內障患者術后應用激素聯合非甾體抗炎藥治療的臨床效果。方法將200例白內障患者隨機分為觀察組(妥布霉素地塞米松+普拉洛芬)和對照組(妥布霉素地塞米松),每組100例,觀察記錄患者圍治療期的各項癥狀和體征的評分及綜合評分。結果觀察組黃斑囊樣水腫發生率和前房閃輝評分明顯小于對照組,差異有統計學意義(P<0.05),盡管觀察組患者的眼壓評分小于對照組,差異無統計學意義;此外在術后4 d和7 d時[(7.1±0.8)vs(8.3±0.9),(5.2±0.9)vs(6.6±0.7)],觀察組綜合評分顯著低于對照組,差異具有統計學意義(P<0.05),而在術后14 d和30 d時[(3.2±0.7)vs(3.3±0.8),(1.1±0.5)vs(1.1±0.6)],差異無統計學意義。結論白內障患者術后聯用妥布霉素地塞米松和普拉洛芬可以有效地起到早期抗炎和緩解術后不良反應的作用,具有良好的臨床應用價值。
白內障;激素類藥物;非甾體抗炎藥
白內障在眼科治療中普遍使用的手術療法是超聲乳化聯合人工晶體植入術,但是該療法在治療過程中較易使前房發生不同程度的炎癥反應[1]。現階段白內障患者術后抗炎的主要方法即為在患處進行糖皮質激素和非甾體抗炎藥的聯合給藥療法[2],但是對于部分炎癥反應較輕的患者能否進行非激素類藥物給藥治療還有待于進一步研究[3]。本文選取200例白內障患者進行了短期的糖皮質激素和非甾體類抗炎藥聯合給藥,現將結果報道如下。
1 資料與方法
1.1 臨床資料 選取2015年1月~2016年6月在四川省內江市第一人民醫院接受白內障超聲乳化聯合人工晶體植入術治療的200例白內障患者為治療對象,按隨機數字表將其分為對照組和觀察組,每組100例,對照組中有男71例,女29例,年齡51~85歲,平均(68.16±9.75)歲;觀察組中有男64例,女36例,年齡50~89歲,平均(71.35±8.69)歲。兩組臨床資料差異無統計學意義。所有治療對象的準入標準為[4]:(1)年齡相關性白內障患者;(2)眼壓在2.80 kPa以下;(3)診斷未見其他眼科前后節疾病;(4)無糖尿病病史;(5)無眼科手術病史;(6)術中未見并發癥;(7)簽署知情同意書。
1.2 方法 所有患者均由同一組醫護人員進行同等的白內障標準超聲乳化聯合人工晶體植入術進行治療[5],其術后的總療程均為1個月。其中對照組進行常規白內障術后給藥治療:即妥布霉素地塞米松滴眼液,6次/d,連續滴眼4 d,其后改為每天給藥3次;觀察組在進行上述常規給藥的基礎上,同時聯用非甾體類抗炎藥普拉洛芬滴眼液給藥,6次/d,連續滴眼4 d,其后單用普拉洛芬進行給藥,3次/d。
1.3 治療指標 觀察記錄患者圍治療期的各項癥狀和體征變化并進行評分,兩者相加可得綜合評分,觀察方法為在術后4 d、7 d、14 d和30 d分別觀察記錄患者癥狀和體征的治療情況,并檢查測量患者眼底和眼壓的改變情況,對其進行評分的總體范圍為0~4分:無癥狀評0分,輕度癥狀評1分,中度癥狀評2分,重度癥狀評3分,極重癥狀評4分[6]。
1.4 統計學方法 本文實驗數據均采用SPSS 19.0來處理,計量資料采用“±s”表示,組間比較采用t檢驗;計數資料用“n,%”表示,組間比較采用χ2檢驗,P<0.05為差異有統計學意義。
2 結果
2.1 黃斑囊樣水腫 黃斑囊樣水腫患者在觀察組發現1例,對照組發現11例,差異有統計學意義(χ2=8.865,P<0.05)。
2.2 前房閃輝評估 在術后各個檢查時間點,觀察組患者的前房閃輝評分數據均明顯小于對照組,差異有統計學意義(P<0.01)。見表1。
2.3 眼壓評估 在術后各個檢查時間點,觀察組患者的眼壓評分數據均小于對照組,差異無統計學意義。見表2。
2.4 癥狀和體征的綜合評分比較 所有患者治療后的綜合評分均隨著治療時間的增加而降低,在術后4 d和7 d時,觀察組的綜合評分顯著低于對照組,差異具有統計學意義(P<0.05),而在術后14 d和30 d時,差異無統計學意義。見表3。
表1 兩組患者前房閃輝評分比較(±s,pc/ms)Table 1 The comparison between two groups about the scores of anterior chamber flare(±s,pc/ms)

表1 兩組患者前房閃輝評分比較(±s,pc/ms)Table 1 The comparison between two groups about the scores of anterior chamber flare(±s,pc/ms)
項目術后4 d術后7 d術后14 d術后30 d t值7.700 5.108 7.214 3.211觀察組(n=100) 6.3±3.1 6.4±2.7 5.6±2.4 5.5±2.3對照組(n=100) 9.9±3.5 8.5±3.1 8.1±2.5 6.5±2.1 P值<0.01<0.01<0.01<0.05
表2 兩組患者眼壓評分比較(±s,mmHg)Table 2 The comparison between two groups about the scores of intraocular pressure(±s,mmHg)
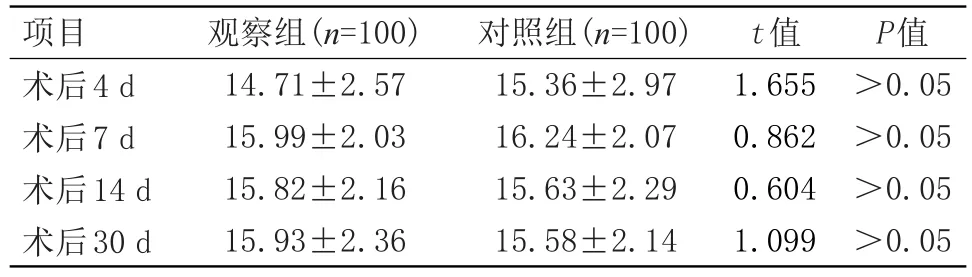
表2 兩組患者眼壓評分比較(±s,mmHg)Table 2 The comparison between two groups about the scores of intraocular pressure(±s,mmHg)
P值>0.05>0.05>0.05>0.05項目術后4 d術后7 d術后14 d術后30 d觀察組(n=100) 14.71±2.57 15.99±2.03 15.82±2.16 15.93±2.36對照組(n=100) 15.36±2.97 16.24±2.07 15.63±2.29 15.58±2.14 t值1.655 0.862 0.604 1.099
表3 兩組患者綜合評分比較(±s,分)Table 3 The comparison between two groups about the comprehensive scores(±s,score)
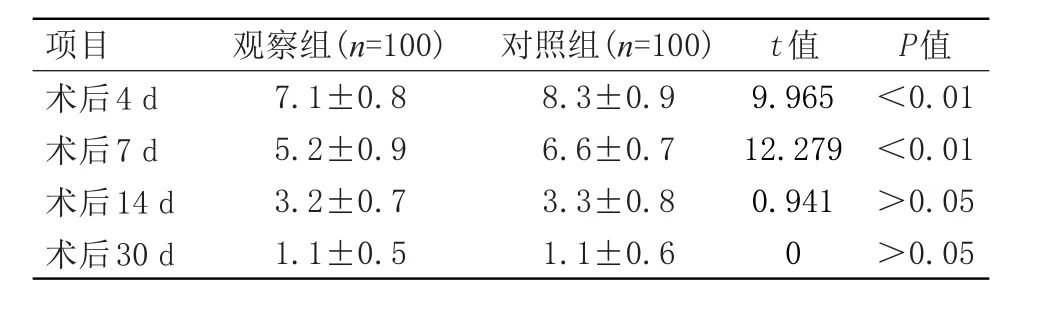
表3 兩組患者綜合評分比較(±s,分)Table 3 The comparison between two groups about the comprehensive scores(±s,score)
P值<0.01<0.01>0.05>0.05項目術后4 d術后7 d術后14 d術后30 d觀察組(n=100) 7.1±0.8 5.2±0.9 3.2±0.7 1.1±0.5對照組(n=100) 8.3±0.9 6.6±0.7 3.3±0.8 1.1±0.6 t值9.965 12.279 0.941 0
3 討論
白內障患者術后炎癥反應的常見影響因素源于手術操作導致的組織器官機械性損傷、超聲能量影響或晶體植入體內后的異物反應等[7],由于物理化學因素會導致前列腺素分泌而對血液房水屏障造成影響和損壞,最終很容易誘發白內障術后炎癥,同時蛋白會極易進入房水內而造成房水閃爍,房水中若出現炎癥細胞等細胞則會引起房水細胞反應,由此可見對該病患者進行術后給藥以控制炎癥的關鍵點為抑制患者前列腺素等細胞因子的作用[8]。一般來講,對此類患者在術后合理應用抗炎藥物則能有效的消退炎癥反應,進而減輕或者治愈超聲乳化術后的前房反應,該療法目前在臨床上已經受到了廣大醫務工作者的普遍認可[9]。
隨著超聲乳化手術的不斷發展完善,臨床上對于白內障患者的術后炎癥反應已經相對大大減輕,因此對于該術式聯合人工晶體植入的患者可縮短糖皮質激素的給藥療程至兩周以內,對于術后未見炎癥反應的患者可以不用糖皮質激素藥物治療[10]。非甾體類抗炎藥在使用中雖可見一定程度的眼壓升高等不良反應,作用效率不如激素類藥物迅速,但其在局部給藥時并不會明顯地損害患者眼角膜上皮細胞,且適應癥更廣泛療效更良好,這就能很較好的彌補長期使用激素類藥物會產生藥物角膜毒性反應的缺憾[11]。本文研究結果與上述文獻報道一致,在術后4天和7天時,觀察組綜合評分顯著低于對照組,差異具有統計學意義(P<0.05),而在術后14天和30天時,差異無統計學意義。
綜上所述,白內障患者術后聯用妥布霉素地塞米松和普拉洛芬可以有效地起到早期抗炎和緩解術后不良反應的作用,具有良好的臨床應用價值。
[1]Hu H,Fang M,Luo K,et al.Phacoemulsification and intraocular lens implantation for cataract induced by ocular ischemic syndrome:30-month follow-up[J]. Jcrs Online Case Reports,2015,3(1):22-26.
[2]Kessel L,Tendal B,J?rgensen KJ,et al.Post-cataract prevention of inflammation and maculared ema by steroid and nonsteroid alanti-inflammatory eye drops: a systematic review[J].Ophthalmology,2014, 121(10):1915-1924.
[3]Malik A,Sadafale A,Gupta YK,et al.A comparative study of various topical nonsteroidal anti-inflammatory drugs to steroid drops for control of post cataract surgery inflammation[J].Oman Journal of Ophthalmology,2016,9(3):150.
[4]黃霞,吳密,陳曉紅.白內障超聲乳化聯合人工晶體植入治療的臨床護理[J].局解手術學雜志,2015,24(1):99-100.
[5]董立紅.超聲乳化聯合人工晶體植入治療超高度近視白內障療效觀察[J].臨床和實驗醫學雜志,2012,11(20):1613-1615.
[6]白景山,張濤,張杰.手術治療白內障對患者臨床癥狀和生活質量的影響[J].現代醫藥衛生,2012,28(19):2921-2922.
[7]Zhang CH,Li N,Wang XY,et al.Influence of Lipoplus fat emulsion on postoperative nutritional status and early inflammatory response in patients with gastrointestinal malignancies[J]. Chinese journal of gastrointestinal surgery,2012,15(5):448-451.
[8]Takács AI,Kovács I,Miháltz K,et al.Central corneal volume and endothelial cell count following femtosecond laser-assisted refractive cataract surgery compared to conventional phacoemulsification[J]. Journal of Refractive Surgery,2012,28(6):387-391.
[9]Ji WJ,Chung BH,Kim EK,et al.The Effects of Two Non-Steroidal Anti-Inflammatory Drugs, Bromfenac 0.1%and Ketorolac 0.45%,on Cataract Surgery[J]. Yonsei Medical Journal,2015,56(6):1671-1677.
[10]Baiula M,Spampinato S.Mapracorat,a Novel Non-Steroidal Selective Glucocorticoid Receptor Agonist for the Treatment of Allergic Conjunctivitis[J].Inflammation&allergy drug targets,2014,13(5):289-298.
[11]Kim SJ,Schoenberger SD,Thorne JE,et al.Topical Nonsteroidal Anti-inflammatory Drugs and Cataract Surgery:A Report by the American Academy of Ophthalmology[J].Ophthalmology,2015,122(11):2159-2168.
Study of the clinical effect about the combination of the drugs hormonal and nonstemidal anti-imqammatory for patients with cataract after operation
Liu Hui,Liu Gang,Luo Li-li
(The First People’s Hospital of Neijiang,Neijiang,Sichuan,641000,China)
ObjectiveTo explore the clinical effect about the combination of the drugs hormonal and nonstemidal anti-imqammatory for patients with cataract after operation.MethodsTwo hundred patients with cataract received operation were divided randomly into the observation group which employed the combination of the drugs tobramycin dexamethasone and pranoprofen and the control group which employed tobramycin dexamethasone.Each group was containing 100 patients.The scores of every symptom,physical sign and general should be statistical record.ResultsAmong two hundred patients with cataract received operation,it is with significantly difference on the cystoid macular edema incidence rate and anterior chamber flare scores between the observation group and the control group,besides,the former numerical value is less than the latter(P<0.05). There is no significantly difference on the intraocular pressure scores between the observation group and the control group although the former numerical value is also less than the latter.In additon,it is with significantly difference on the general scores between the observation group and the control group,besides,the former numerical value is less than the latter after four days and seven days for the operation[(6.3±3.1)vs(9.9±3.5),(6.4± 2.7)vs(8.5±3.1)](P<0.05).There is no significantly difference on the general scores between the observation group and the control group although the former numerical value is also less than the latter after fourteen days and thirty days for the operation[(5.6±2.4)vs(8.1±2.5),(5.5±2.3)vs(6.5± 2.1)].Conclusion It is effective and valuable to resist inflammatory and adverse reaction with the combination of the drugs tobramycin dexamethasone and pranoprofen for patients with cataract after operation.
Cataract;Hormonal drugs;Nonstemidal anti-imqammatory drugs
10.3969/j.issn.1009-4393.2017.11.007
猜你喜歡
英語世界(2023年10期)2023-11-17 09:19:16
汽車實用技術(2022年10期)2022-06-09 11:16:58
音樂探索(2022年2期)2022-05-30 21:01:37
收藏界(2019年3期)2019-10-10 03:16:40
小天使·一年級語數英綜合(2019年8期)2019-08-27 02:23:00
中國特種設備安全(2018年11期)2019-01-08 02:08:32
小學科學(學生版)(2018年7期)2018-08-13 09:33:04
中國非營利評論(2017年1期)2017-11-09 03:09:10
海外華文教育(2017年8期)2017-11-07 04:42:02
現代語文(2016年21期)2016-05-25 13:13:50