性別對老年髖關節骨折患者術后并發癥影響的臨床研究
2017-09-21 01:58:37杜小平張在謙常浩勝劉利軍王延軍
創傷外科雜志 2017年9期
關鍵詞:研究
杜小平,張在謙,常浩勝,劉利軍,王延軍
·論 著·
性別對老年髖關節骨折患者術后并發癥影響的臨床研究
杜小平,張在謙,常浩勝,劉利軍,王延軍
目的評估性別對老年髖關節骨折患者術后并發癥之間關系。方法選取自2012年1月—2015年1月就診的髖關節骨折老年患者(>65歲)130例,記錄其骨折前基礎情況、術后并發癥以及病死率情況。分析性別之間的差異,采用Logistic回歸分析影響并發癥發生的可能因素。結果納入的研究對象中男性40例,女性90例,兩組年齡、美國麻醉醫師協會標準(ASA)評分、基礎疾病等一般情況無統計學差異(P>0.05)。術后男性與女性比并發癥以心血管疾病(17.5%vs. 13.3%,χ2=5.110,P=0.024)及肺炎(12.5%vs. 5.6%,χ2=6.430,P=0.011)多見,女性與男性相比泌尿系統感染較多(31.1%vs. 20.0%,χ2=4.464,P=0.035)。在術后4個月內男性病死率較女性高(25.0%vs. 13.3%,χ2=5.110,P=0.024)。認知功能障礙是壓瘡、心血管疾病、肺炎等并發癥的危險因素(OR值分別為1.4(95%CI:1.1,1.8)、1.5(95%CI:1.1,1.9)、2.3(95%CI:1.5,3.7)]。結論老年髖關節骨折患者中多伴有基礎疾病,男性術后肺部及心血管并發癥的發病率以及術后病死率較高。
髖關節骨折; 性別; 并發癥
社會老齡化的發展,高齡患者骨折的發病率越來越高,髖部是老年人骨折的好發部位,手術是治療方法的首選[1-2]。老年人多常伴有基礎性疾病,術后發生并發癥或者死亡的概率明顯增加[3-6]。已有研究發現男性伴有基礎疾病會導致術后感染發病率增高,出現呼吸系統、循環系統等疾病導致死亡[7-8]。Endo等[9]研究發現術前伴發基礎疾病的數目與性別無關,但是根據美國麻醉醫師協會標準(American Society of Anesthesiologists,ASA),男性術后并發癥發生率比例較高。該研究分析性別對髖關節骨折患者術后4個月內短期并發癥方面的影響,并研究影響并發癥的相關因素。
資料與方法
1研究對象
選取2012年1月—2015年1月就診于榆林市中醫醫院北方醫院的髖關節骨折患者150例為研究對象。排除標準:(1)年齡<65歲;(2)病理性骨折者,如轉移瘤所致骨折、良惡性骨腫瘤等引起的骨折。根據指南確定患者診療方案[10],圍手術期嚴格限制泌尿導管的使用,術后鼓勵患者早期功能鍛煉。
2臨床資料
以患者骨折前4個月內身體狀況及精神狀況為基線。基礎疾病分為心血管疾病、卒中、肺部疾病、腎臟疾病、糖尿病、風濕性疾病、帕金森病和惡性腫瘤。吸煙分為吸煙及不吸煙者。根據Katz活動評分進行評估[10];根據歐洲髖部骨折的標準化評價(standardised audit of hip fractures in Europe,SAHFE)確定髖關節骨折類型[11];根據ASA評分評估患者身體狀況[12];根據智力狀態問卷(short portable mental status questionnaire,SPMSQ)評估患者精神狀況,其中認知功能紊亂分為正常(≥8分)、輕(6~7分)、中(3~5分)、重(0~2分)[13],本試驗中認知功能障礙分為無(≥8分)和有(≤7分)。并發癥主要包括:肺炎、心血管疾病、深靜脈血栓形成、肺栓塞、切口感染、泌尿系統感染、消化道出血、腦血管病變、壓瘡。
3統計學分析
結 果
1研究對象基本資料對比
老年髖關節骨折150名患者排除年齡<65歲(9例)、病理性骨折(7例)、失訪(4例),最終研究對象為130例患者,其中男性40例,女性90例。基線資料主要包括人口學資料、骨折類型和機體狀況,研究對象基線資料差異無統計學意義。見表1。
2性別與并發癥及病死率關系
男女組患者中并發癥發生率分別為56.9%和57.5%(P>0.05),差異無統計學意義。但肺部感染、泌尿系統感染及心血管并發癥差異有統計學意義,余無統計學意義。女性和男性30d內病死率為10.0%和17.5%,4個月內病死率為13.3%和25.0%,差異有統計學意義(P<0.05)。見表2。
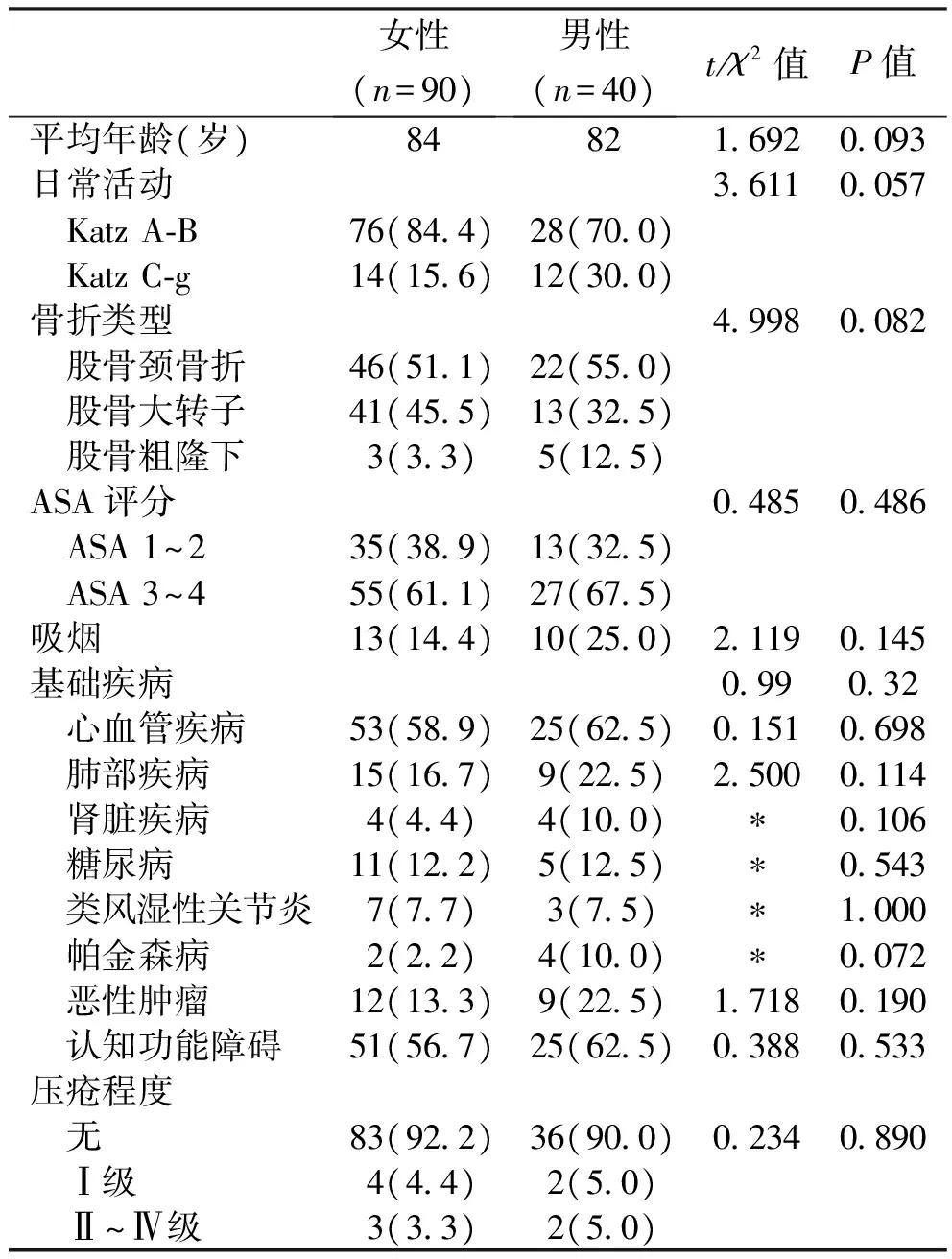
表1 髖關節骨折患者臨床資料[n(%)]
*Fisher精確概率法計算P值

表2 髖關節骨折患者并發癥[n(%)]
*Fisher精確概率法計算P值
3并發癥影響因素分析
性別、年齡、ASA、心血管疾病、肺部疾病、認知障礙與壓瘡、心血管疾病、肺炎這三類主要的并發癥之間存在相關性,其中女性心血管并發癥與肺炎并發癥高于男性[(OR值分別為1.3(95%CI:1.0~1.8)、2.8(95%CI:1.8~3.7)],年齡≥80歲的患者發生壓瘡的可能性高于<80歲的患者(OR=1.4,95%CI:1.1~1.8),ASA評分3~4級的患者三類并發癥發生率明顯高于評分在1~2級的患者(OR值分別為1.3(95%CI:1.1~1.5)、2.3(95%CI:1.5~3.2)、2.6(95%CI:1.5~3.8)。部分基礎疾病的患者并發癥發生率更高。認知功能障礙是壓瘡、心血管疾病、肺炎等并發癥的危險因素(OR值分別為1.4(95%CI:1.1~1.8)、1.5(95%CI:1.1~1.9)、2.3(95%CI:1.5~3.7)。見表3。
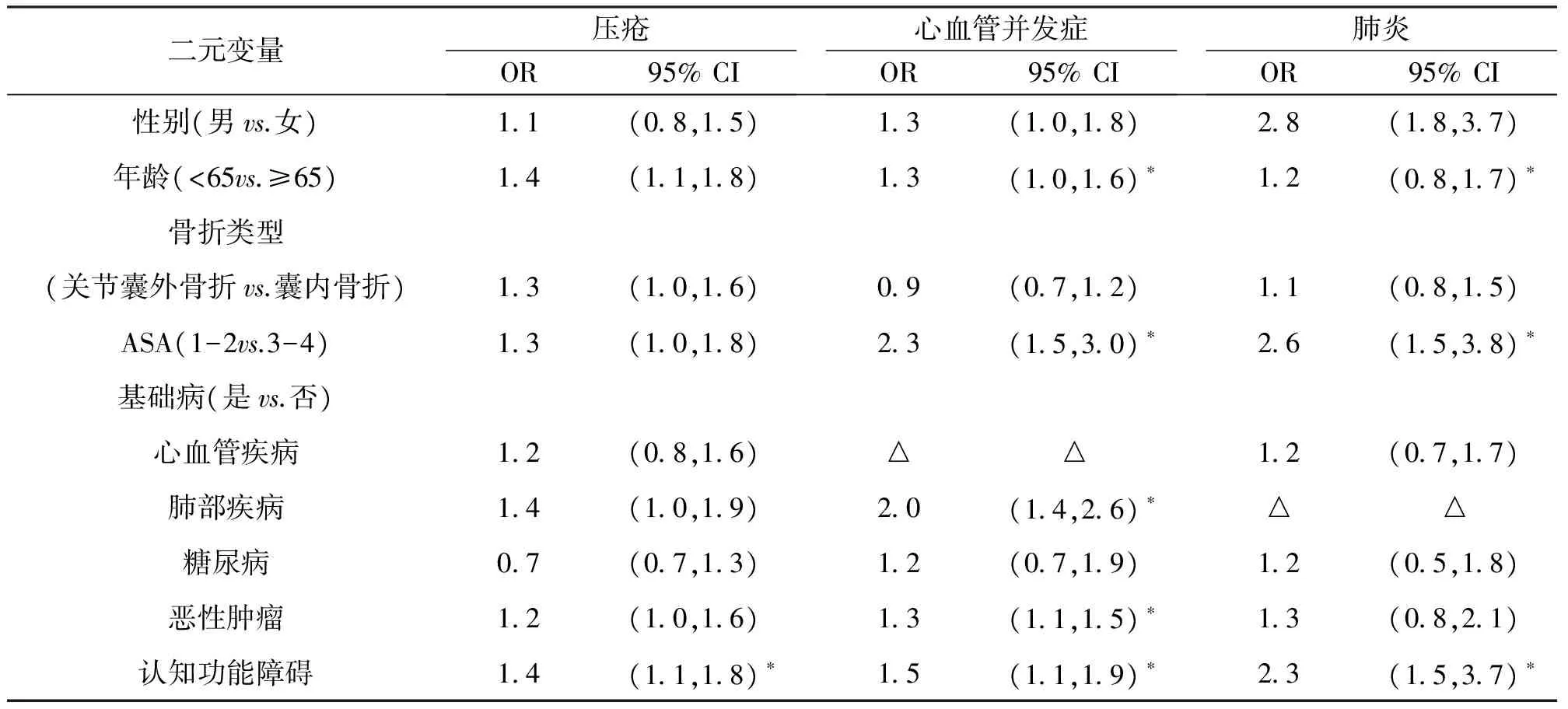
表3 相關變量對壓瘡、肺炎及心血管并發癥影響
*P<0.05;△:該因素與該并發癥同類,無法計算OR
討 論
老年人發生髖關節骨折后往往預后較差,其致殘率及病死率均較高[14-16]。有研究表明,嚴重認知功能障礙會導致髖關節骨折術后患者病死率提高,輕度認知功能障礙會導致會導致并發癥的發生率增加[17-18]。大量研究表明髖關節骨折后最常見的術后并發癥是感染和心血管系統疾病,其中泌尿系統感染最為常見[5,19-20]。此外,Youm等[21]研究報道吸煙與并發癥的發生無關。
本研究結果表明,男性髖關節骨折患者術后肺部及心血管并發癥發生率高。在一定程度上認知功能障礙會導致并發癥的發生,因此評估性別與心肺疾病及認知功能方面的影響可以減少并發癥的發生。與類似研究相比,本研究中并發癥的發生率較高,可能是研究中未排除認知功能障礙患者。研究結果表明認知障礙會增加壓瘡、肺部感染、心血管等并發癥的發生,因此髖關節骨折患者應盡早評估患者精神狀態。感染及心血管并發癥是常見的術后并發癥,男性因肺炎所致的病死率較女性高(4個月內病死率,25.0%vs. 13.3%,P<0.05),因此在評估患者發生肺炎等嚴重并發癥時需要考慮性別因素。試驗中4個月的隨訪時間內泌尿系統感染發生率比之前研究高[22]。有研究表明縮短手術時間對患者手術后恢復自理功能、減少并發癥十分重要[23]。但對于伴有心血管基礎疾病患者,圍手術期需要心血管系統達到最佳狀況,會增加術前準備時間,因此需要平衡心血管疾病術前準備時間。本試驗存在局限性:(1)研究內容未涉及患者目前藥物治療方案、實驗室指標及繼發性骨質疏松等可能會增加患者病死率的因素;(2)試驗中研究對象失訪會影響試驗結果;(3)試驗樣本包含認知功能障礙者,而認知功能障礙通常是髖關節骨折患者術前研究的排除標準之一。
綜上所述,老年髖關節骨折患者中多伴有基礎疾病,男性術后肺部及心血管并發癥的發病率較高,女性泌尿系統感染發病率較高。對髖關節骨折患者,應該從性別角度出發,并結合基礎疾病和認知功能障礙情況,積極預防并發癥的發生。
[1] Shah MR,Aharonoff GB,Wolinsky P,et al.Outcome after hip fracture in individuals ninety years of age and older[J].Orthop Trauma,2001,15(1):34-39.
[2] L?fgren S,Ljunggren G,Brommels M.No ticking time bomb:hospital utilisation of 28,528 hip fracture patients in Stockholm during 1998-2007[J].Scand J Public Health,2010,38(4):418-425.
[3] 張志勇,侯曉華,解光越,等.老年髖部骨折與骨質疏松的相關性分析[J].中華流行病學雜志,2012,33(12):1293-1295.
[4] Merchant RA,Lui KL,Ismail NH,et al.The relationship between postoperative complications and outcomes after hip fracture surgery[J].Ann Acad Med Singapore,2005,34(2):163-168.
[5] 鄧忠光.手術治療老年髖部骨折110例療效分析[J].中國現代藥物應用,2010,4(9):66-67.
[6] 張禹,王琦,高波,等.不同類型老年髖部骨折術后生存率和功能結果的臨床研究[J].中原醫刊,2008,35(5):25-27.
[7] Wehren LE,Hawkes WG,Orwig DL,et al.Gender differences in mortality after hip fracture:the role of infection[J].Bone Miner Res,2003,18(12):2231-2237.
[8] Panula J,Pihlajam?ki H,Mattila V,et al.Mortality and cause of death in hip fracture patients aged 65 or older.A population based study[J].BMC Musculoskelet Disord,2011,12:105-106.
[9] Endo Y,Aharonoff GB,Zuckerman JD,et al.Gender differences in patients with hip fracture:a greater risk of morbidity and mortality in men[J].Orthop Trauma,2005,19(1):29-35.
[10] Wamala S,Holm LE.Swedish National Institute of Public Health and the National Board of Health and Welfare reply: we will inform about the risks[J].Lakartidningen,2010,107(1-2):46-47.
[11] Parker MJ,Currie CT,Thorngren KG.Standardised audit of hip fractures in Europe[J].Hip Int,1998,8:10-15.
[12] Owens WD,Felts JA,Spitznagel EL Jr.ASA physical status classifications:a study of consistency of ratings[J].Anesthesiology,1978,49(4):239-243.
[13] Pfeiffer E.A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients[J].Am Geriatr Soc,1975,23(10):433-441.
[14] 肖紅兵,胡有忠.應用綜合手術治療老年人髖部骨折的臨床研究[J].中國社區醫師:醫學專業,2010,12(33):65.
[15] 閆軍,曹步霞,徐瓊,等.高齡髖部骨折患者常見并發癥原因及預防對策[J].中國實用醫藥,2010,(1):67-68.
[16] Giusti A,Barone A,Razzano M,et al.Predictors of hospital readmission in a cohort of 236 elderly discharged after surgical repair of hip fracture:one-year follow-up[J].Aging Clin Exp Res,2008,20(3):253-259.
[17] S?derqvist A,Ekstr?m W,Ponzer S,et al.Prediction of mortality in elderly patients with hip fractures:a two-year prospective study of 1,944 patients[J].Gerontology,2009,55(5):496-504.
[18] Stromberg L,Lindgren U,Nordin C,et al.The appearance and disappearance of cognitive impairment in elderly patients during treatment for hip fracture[J].Scand J Caring Sci,1997,11(3):167-175.
[19] 李玉明.老年髖部骨折并發癥的預防及康復護理[J].中國醫藥導報,2010,7(22):158-160.
[20] Roche JJ,Wenn RT,Sahota O,et al.Effect of comorbidities and postoperative complications on mortality after hip fracture in elderly people:prospective observational cohort study[J].BMJ,2005,331(7529):1374.
[21] Youm T,Aharonoff G,Zuckerman JD,et al.Effect of previous cerebrovascular accident on outcome after hip fracture[J].Orthop Trauma,2000,14(5):329-334.
[22] Norris R,Parker M.Diabetes mellitus and hip fracture:a study of 5,966 cases[J].Injury,2011,42(11):1313-1316.
[23] Khan SK,Kalra S,Khanna A,et al.Timing of surgery for hip fractures:a systematic review of 52 published studies involving 291,413 patients[J].Injury,2009,40(7):692-697.
(本文編輯: 郭 衛)
Effectofgenderonthepostoperativecomplicationsafterhipfracturesurgery
DUXiao-ping1,ZHANGZai-qian1,CHANGHao-sheng1,LIULi-jun1,WANGYan-jun2
(1.Department of Orthopedics,Traditional Chinese Medicine Hospital of Yulin,Yulin,Shanxi 718000; 2.Department of Orthopaedics,Xi’an Daxing Hospital,Xi’an 710016,China)
ObjectiveTo assess the relationship between gender and postoperative complications in elderly patients with hip fracture.MethodsTotally 130 elderly patients (>65 years old) with hip fracture were selected as the research object,who were admitted and treated in our hospital from Jan. 2012 to Jan. 2015. The basic condition before fracture,complications and mortality after operation were recorded. The difference between men and women was analyzed,and Multiple Logistic Regression was used to analyze the factors affecting complications.ResultsThere were 90 female patients and 40 male patients. There was no statistical difference in age,ASA grade and basic diseases between the two groups(P>0.05). Comparing with female,the postoperative complications of male patients were mainly cardiovascular complications (17.5%vs. 13.3%,χ2=5.110,P=0.024) and pneumonia (12.5%vs. 5.6%,χ2= 6.430,P= 0.011),but females got urethral infection easily (31.1%vs. 20.0%,χ2=4.464,P=0.035). Within 4 months after the operation,the mortality of male patients was higher than females (25.0%vs. 13.3%,χ2=5.110,P=0.024). Cognitive dysfunction was a risk factor for bedsore,cardiovascular disease and pneumonia(OR was 1.4 (95%CI:1.1-1.8),1.5 (95%CI: 1.1-1.9),2.3 (95%CI:1.5-3.7),respectively).ConclusionThe elderly patients with hip fractures often accompany with a lot of basic diseases. After operation,male patients are more likely to get pulmonary and cardiovascular complications,and their postoperative mortality is higher than females.
hip fracture; gender; complications
718000 陜西,榆林市中醫醫院北方醫院骨一科(杜小平,張在謙,常浩勝,劉利軍); 710016 西安,西安大興醫院骨一科(王延軍)
張在謙,E-mail:543718037@qq.com
1009-4237(2017)09-0677-04
R 681.6
A
10.3969/j.issn.1009-4237.2017.09.009
2016-02-27;
2017-01-12)
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
天津外國語大學學報(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
科技傳播(2019年22期)2020-01-14 03:06:54
遼金歷史與考古(2019年0期)2020-01-06 07:45:20
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
電子制作(2018年11期)2018-08-04 03:26:04
汽車工程學報(2017年2期)2017-07-05 08:13:02
國際商務財會(2017年8期)2017-06-21 06:14:14
電子制作(2017年23期)2017-02-02 07:17:19