絕經后女性肌少癥與頸動脈斑塊發生風險的關系
2024-07-10 12:07:16戈凌霞馮健吳良玉劉琴朱小賢夏青
護理研究 2024年13期
關鍵詞:影響因素
戈凌霞 馮健 吳良玉 劉琴 朱小賢 夏青
基金項目 上海市加強公共衛生體系建設三年行動計劃(2023-2025年)項目,編號:GWVI?11.1?28
作者簡介 戈凌霞,主管護師,本科
通訊作者 夏青,E?mail:1034441245@qq.com
引用信息 戈凌霞,馮健,吳良玉,等.絕經后女性肌少癥與頸動脈斑塊發生風險的關系[J].護理研究,2024,38(13):2276?2280.
Relationship between sarcopenia and carotid plaque risk in post?menopausal women
GE Lingxia, FENG Jian, WU Liangyu, LIU Qin, ZHU Xiaoxian, XIA Qing
Health Examination Center of Shanghai Health and Medical Center(Huadong Sanatorium), Jiangsu 214065 China
Corresponding Author? XIA Qing, E?mail: 1034441245@qq.com
Abstract? Objective:To investigate the relationship between sarcopenia and the risk of carotid plaque in postmenopausal women.Methods:A total of 527 postmenopausal women who underwent physical examination in the health examination center of Huadong Sanatorium from March to October 2022 were selected as the research objects by random cluster sampling.The body composition analyzer (InBody720) was used to calculate the skeletal muscle mass of human limbs, appendicular skeletal muscle index (ASMI) was calculated and handgrip and walking speed were measured. Clinical data were collected, univariate combined with multivariate regression analysis was used to explore the relationship between sarcopenia and the risk of carotid plaque in postmenopausal women,and receiver operating characteristic (ROC) curve was used to explore the diagnostic value of ASMI in the occurrence of carotid plaque in postmenopausal women.Results:Among 527 postmenopausal women, 172 (32.6%) had carotid plaque. In postmenopausal women, ASMI in the carotid plaque group was significantly lower than that in the non-carotid plate group [5.42(4.88,6.09)kg/m2 vs 6.63(5.73,7.78)kg/m2,P<0.001]. The incidence of sarcopenia in the carotid plaque group was significantly higher than that in the non-carotid plaque group (45.3% vs 18.0%, P<0.001).The lower the ASMI value in postmenopausal women,the higher the risk of carotid plaque (Pfor trend<0.001).Multivariate logistic regression analysis showed that postmenopausal women with sarcopenia significantly increased the risk of carotid plaque(OR=3.486,95%CI 2.237-5.432). ROC showed that ASMI had a higher predictive value for carotid plaque than waist circumference and body mass index (AUC=0.756).Conclusions:Sarcopenia significantly increases the risk of carotid artery plaque in postmenopausal women,and ASMI can be used as a simple predictor of carotid artery plaque.
Keywords??? postmenopausal; carotid artery plaque; sarcopenia; appendicular skeletal muscle index, ASMI; influencing factors;prediction
摘要? 目的:探討絕經后女性肌少癥與頸動脈斑塊發生風險的相關性。方法:采用整群抽樣法,選取2022年3月—10月在華東療養院體檢中心進行健康體檢的絕經后女性527例為研究對象。采用人體成分分析儀(InBody720)檢測人體四肢骨骼肌質量,計算四肢骨骼肌指數(ASMI)并測量握力與步速。收集一般資料及實驗室指標,采用多因素Logistic回歸分析探討絕經后女性肌少癥與頸動脈斑塊發生風險的關系,并采用受試者工作特征(ROC)曲線探討ASMI對頸動脈斑塊發生的預測價值。結果:527例絕經后女性中,172例發生頸動脈斑塊,發生率為32.6%。絕經后女性頸動脈斑塊組ASMI低于非頸動脈斑塊組[5.42(4.88,6.09)kg/m2與 6.63(5.73,7.78)kg/m2,P<0.001],同時頸動脈斑塊組肌少癥發生率顯著高于非頸動脈斑塊組(45.30%與18.00%,P<0.001)。絕經后女性ASMI越小,頸動脈斑塊發生風險越高(Pfor trend<0.001)。多因素Logistic回歸分析顯示,肌少癥增加絕經后女性頸動脈斑塊發生風險[OR=3.486,95%CI(2.237,5.432)]。ROC分析顯示,相比于腰圍及體質指數,ASMI對頸動脈斑塊有更高的預測價值(ROC曲線下面積=0.756)。結論:絕經后女性肌少癥增加其頸動脈斑塊發生風險,ASMI可作為預測其頸動脈斑塊發生的簡易指標。
關鍵詞? 絕經后女性;頸動脈斑塊;肌少癥;四肢骨骼肌指數;影響因素;預測
doi:10.12102/j.issn.1009-6493.2024.13.004
亞洲肌少癥工作組在2020年發布的《肌少癥診斷、治療2019更新版共識》中指出,肌少癥是與增齡有關的進行性全身肌肉減少和/或肌肉強度下降或肌肉生理功能減退的癥狀[1]。肌少癥涉及多種風險因素及機制,包括遺傳、營養、運動、神經功能、肌細胞凋亡及機體激素變化情況[2]。而肌少癥在絕經后女性群體中發生率較高,據統計,有31%的絕經后女性出現肌少癥[3],由于雌激素水平顯著下降會導致代謝功能紊亂,同時影響骨骼肌的肌蛋白合成[4]。同時有研究顯示,絕經后女性頸動脈粥樣硬化或斑塊形成的發生同樣顯著增高,可能與雌激素缺乏導致血管保護發生紊亂有關[5?6]。而肌少癥與機體代謝異常也密切相關,既往有研究證實肌少癥會增加糖尿病人群頸動脈粥樣硬化發生風險[7],而目前尚未檢索到相關研究證實肌少癥會增加絕經后女性人群頸動脈斑塊的發生風險,絕經后女性隨著脂肪質量和分布發生改變,其肥胖指標如體重指數和腰圍也會發生相應變化,同時過度肥胖會顯著增加頸動脈斑塊的發生風險,也未檢索到肌少癥與肥胖指標對絕經后女性發生頸動脈斑塊預測價值的比較相關研究。因此,本研究擬探討絕經后女性肌少癥與頸動脈斑塊發生風險的相關性,旨在對絕經后女性早期進行肌少癥干預、預防頸動脈斑塊發生提供參考。
1? 對象與方法
1.1 研究對象
采用整群抽樣法,選取2022年3月—10月在華東療養院體檢中心進行常規健康體檢的絕經后女性527人,年齡40~88(55.13±9.77)歲。排除標準:嚴重肝、腎功能不全;手術或意外因素導致突然停經;無法獨立完成調查;患有骨關節疾病(腰椎間盤突出、類風濕關節炎)或骨骼肌損傷;基本健康體檢信息不全。本研究取得病人知情同意,并經華東療養院倫理委員會審核通過。
1.2 資料收集
1.2.1 基線資料
基礎資料包括年齡、腰圍(WC)、體重指數(BMI)、收縮壓、舒張壓[8]。
1.2.2 實驗室檢查指標
采集體檢者清晨空腹靜脈血10~15 mL,實驗室檢查包括空腹血糖(FBG)、三酰甘油(TG)、總膽固醇(TC)、低密度脂蛋白膽固醇(LDL?C)、高密度脂蛋白膽固醇(HDL?C)、白細胞計數(WBC)、中性粒細胞計數(NE)、淋巴細胞計數,并計算中性粒細胞/淋巴細胞百分比(NLR)。所有實驗室指標均在采樣后24 h內于華東療養院醫學檢驗中心進行檢驗。
1.3 診斷標準
1.3.1 肌少癥
采用InBody720多頻生物電阻抗人體成分分析儀對研究對象進行四肢骨骼肌評估,受試者禁食、禁飲8 h,排空大小便。研究對象赤足站立于電極板上,雙手握住電極,分析儀自動計算四肢骨骼肌質量。四肢骨骼肌指數(ASMI)=四肢骨骼肌質量(kg)/[身高(m)]2;測量研究對象優勢手握力,采用奧匹握力測試儀(AP?1005)進行握力測試,間隔30 s,連續測量3次取最大值;采用6 m行走距離測量其步速,連續測量3次取最大值。肌少癥按照2016年中華醫學會骨質疏松和骨礦鹽疾病分會制定的肌少癥相關共識診斷,將ASMI<5.7 kg/m2,女性握力≤18 kg且步速低于0.8 m/s作為肌少癥診斷標準[9]。
1.3.2 頸動脈斑塊
采用美國GELogiqE9超聲診斷儀檢測頸動脈血管情況。研究對象取仰臥位,頭偏向檢查側對側,充分暴露頸部區域,超聲探頭依次沿著頸總動脈端、分叉處以及頸內動脈、頸外動脈起始處的內膜中層厚度進行掃描,頸動脈內膜中層厚度≥1.5 mm診斷為頸動脈斑塊形成[10]。
1.3.3 糖尿病
根據《中國肥胖及2型糖尿病外科治療指南(2019版)》對2型糖尿病的定義,即空腹血糖(FBG)≥7.0 mmol/L或糖化血紅蛋白≥6.5%即診斷為糖尿病[11]。
1.3.4 高血壓
根據《中國高血壓防治指南(2018年修訂版)》定義,高血壓指收縮壓≥140 mmHg和(或)舒張壓≥90 mmHg[12]。
1.4 統計學方法
采用SPSS 24.0軟件進行統計分析,定量資料符合正態分布,采用均數±標準差(x±s)描述,組間比較采用t檢驗,非正態分布的定量資料采用中位數、四分位數[M(P25,P75)]描述,組間比較采用秩和檢驗;定性資料以例數、百分比(%)表示,組間比較采用χ2檢驗。采用趨勢性檢驗分析ASMI不同四分位區間與頸動脈斑塊發生風險的關系。采用多因素Logistic回歸分析探討絕經后女性肌少癥與頸動脈斑塊發生的關系。采用受試者工作特征曲線(ROC)評估ASMI、腰圍及BMI對頸動脈斑塊發生的預測價值。P<0.05為差異有統計學意義。
2? 結果
2.1 絕經后女性頸動脈斑塊發生風險影響因素的單因素分析
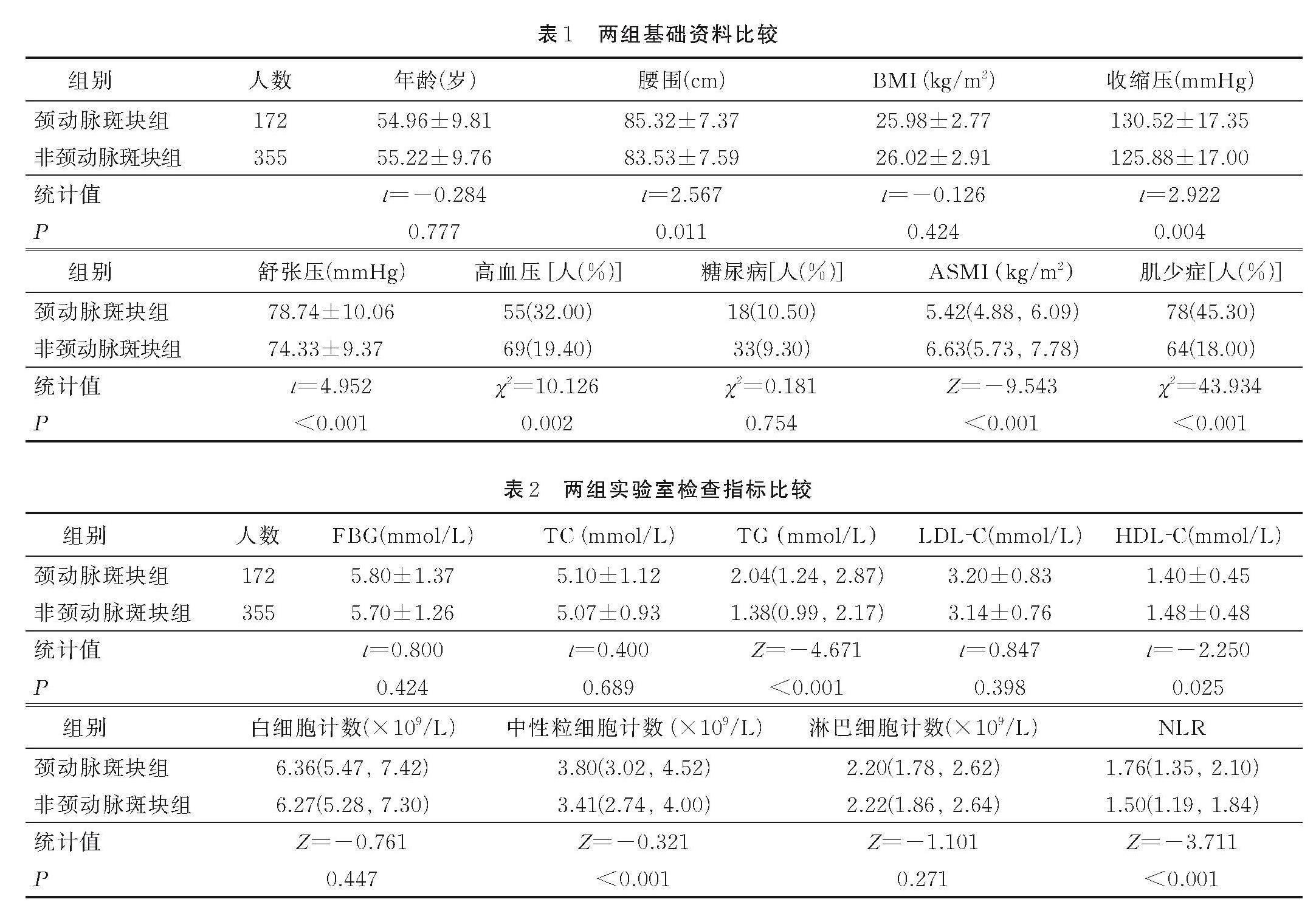
本研究共納入527名絕經后女性,172人發生頸動脈斑塊,發生率為32.6%。頸動脈斑塊組肌少癥發生率(45.30%)高于非頸動脈斑塊組(18.00%),差異有統計學意義(χ2=43.934,P<0.001)。單因素分析結果見表1、表2。
2.2 絕經后女性ASMI不同數值區間與頸動脈斑塊發生風險的關系
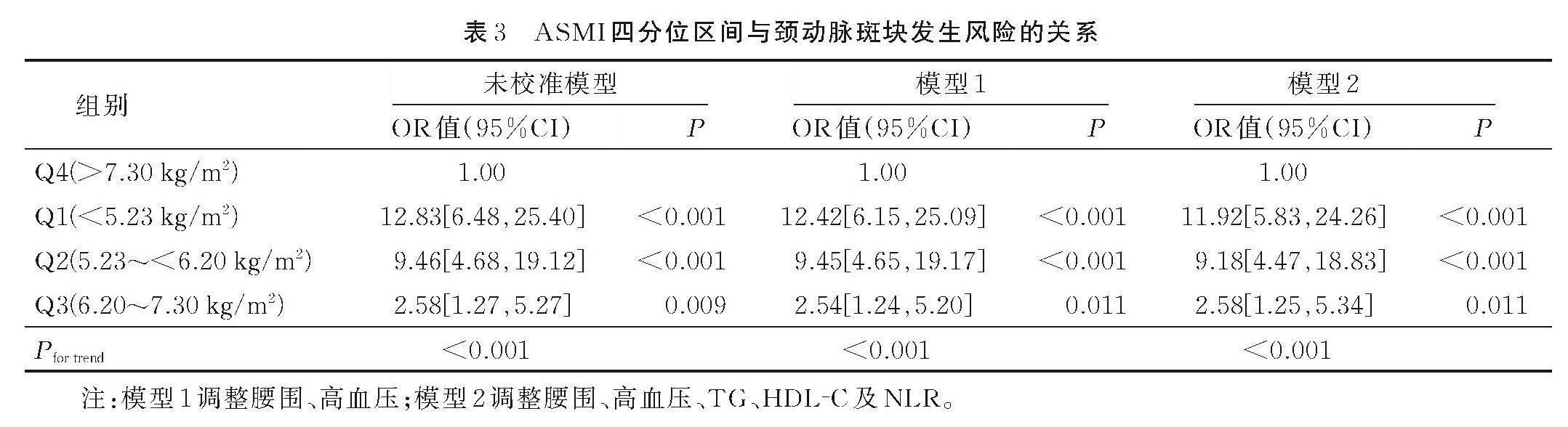
根據ASMI四分位區間劃分Q1、Q2、Q3及Q4共4個區間,結果顯示,調整腰圍、高血壓、TG、HDL?C及NLR等混雜因素后,以Q4為參照組,結果顯示,Q1[OR=11.92,95%CI(5.83,24.26)]、Q2[OR=9.18,95%CI(4.47,18.83)]及Q3[OR=2.58,95%CI(1.25,5.34)]絕經后女性頸動脈斑塊發生風險均增加(P<0.05),且隨著ASMI數值的降低,其頸動脈斑塊發生風險也顯著增加(Pfor trend<0.001)。見表3。
2.3 絕經后女性頸動脈斑塊發生風險影響因素的多因素Logistic回歸分析
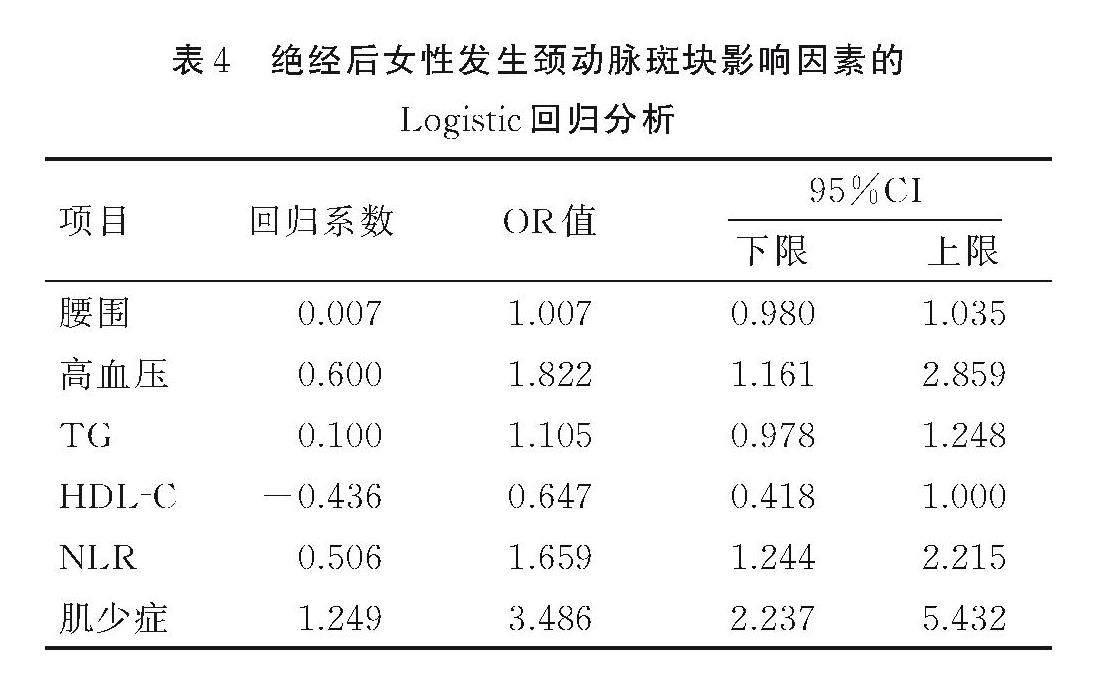
將腰圍、TG、HDL?C、NLR(連續變量以實際值賦值)和高血壓(否=0,是=1)、肌少癥(否=0,是=1)作為自變量,以絕經后女性是否發生頸動脈斑塊為因變量(否=0,是=1)進行多因素Logistic回歸分析。結果顯示,肌少癥是絕經后女性發生頸動脈斑塊的獨立危險因素[OR=3.486, 95%CI(2.237,5.432)]。見表4。
2.4 ASMI、BMI及腰圍對絕經后女性頸動脈斑塊發生風險的預測價值
進一步比較ASMI、腰圍及BMI對絕經后女性發生頸動脈斑塊的預測價值,結果顯示,相較于腰圍及BMI,絕經后女性ASMI對頸動脈斑塊發生的預測價值更高,其ROC曲線下面積(AUC)為0.756,靈敏度為83.70%,特異度為72.50%,Youden指數為0.562。見圖1、表5。
3? 討論
絕經后女性由于卵巢功能衰退,其所分泌的性激素也顯著下降,既往研究已經證實雌激素對心血管及骨骼肌組織生理活性具有重要作用[13?14]。女性在50歲后肌肉質量會顯著下降,絕經后女性的肌肉組織以每年0.6%遞減,尤其在絕經后3年內,肌肉量下降速度最快[15?17]。由于雌激素與睪酮水平隨著年齡的增長逐漸下降,其在肌肉組織的代謝和合成中的作用不斷降低,而研究表明絕經后女性睪酮水平降低比較緩慢,對其肌肉量影響較小[18]。因此,絕經后女性肌肉量減少主要與雌激素降低密切相關。在肌肉細胞膜、細胞質及細胞核上均有雌激素受體[19?20],通過胰島素樣生長因子?1(insulin?like growth factor 1,IGF?1)等途徑影響肌肉蛋白質合成[21]。同時有研究表明,絕經后女性存在血管內皮依賴性和非依賴性舒張功能障礙,導致頸動脈內膜中層增厚及斑塊的形成[22?24]。這可能與絕經后女性雌激素下降導致脂質代謝異常有關。研究表明,雌二醇可降低絕經后女性脂蛋白水平,減少腦血管栓塞的發生。除了雌激素對血脂的調節功能,還有研究顯示雌激素可抑制內皮細胞黏附分子的表達,促進一氧化氮的合成,減少平滑肌細胞增殖,抑制趨化物質和單核細胞的化學吸附作用,并降低纖維蛋白原合成[5, 25]。隨著絕經后雌激素的降低,雌激素對血脂調節功能下降,對血管保護作用不斷降低,其頸動脈斑塊發生風險也不斷增高。
多因素回歸分析顯示,絕經后女性肌少癥顯著增加頸動脈斑塊發生風險(OR=3.486)。由于肌少癥與頸動脈粥樣斑塊形成具有一些共同的病理生理機制,其中包括機體慢性炎癥、胰島素抵抗及增齡等。慢性炎癥產生大量炎性細胞因子及增齡導致的細胞氧化應激作用會促進血管內皮細胞功能紊亂,并加速血管粥樣斑塊形成[26]。而骨骼肌作為胰島素作用的重要場所,胰島素抵抗會導致肌肉蛋白的合成速度顯著下降,并增加肌蛋白分解,造成肌肉組織大量流失[27]。同時,胰島素抵抗會引起脂質代謝和血管內皮細胞紊亂,進一步加劇動脈粥樣硬化的發生[28?29]。增齡也會促進肌肉組織減少并伴有內臟等異位脂肪堆積[30]。高齡人群脂代謝與糖代謝會進一步加劇肥胖形成,肥胖人群也成為頸動脈斑塊發生的高危人群[31]。而既往研究尚未探索絕經后女性肥胖指標與肌少癥預測頸動脈斑塊形成的差異,而本研究顯示ASMI在絕經后女性頸動脈斑塊的診斷價值要優于腰圍及BMI,提示肌少癥人群可能比肥胖人群更容易出現頸動脈斑塊。
4? 小結
綜上所述,絕經后女性可能由于雌激素水平下降或伴有脂代謝異常及增齡因素,導致肌少癥發生率顯著增加,肌少癥產生的同時會顯著增加其頸動脈斑塊發生風險,臨床應重點干預絕經后肌少癥人群,降低其頸動脈斑塊發生風險。
參考文獻:
[1]? CHEN L K,WOO J,ASSANTACHAI P,et al.Asian Working Group for Sarcopenia:2019 consensus update on sarcopenia diagnosis and treatment[J].Journal of the American Medical Directors Association,2020,21(3):300-307.
[2]? 于寶海,吳文娟.2018歐洲肌少癥共識解讀[J].河北醫科大學學報,2019,40(4):373-379;384.
YU B H,WU W J.Interpretation of 2018 European myopenia consensus[J].Journal of Hebei Medical University,2019,40(4):373-379;384.
[3]? PAP Z,KALABISKA I,BALOGH ?,et al.Prevalence of sarcopenia in community dwelling outpatient postmenopausal Hungarian women[J].BMC Musculoskeletal Disorders,2022,23(1):207.
[4]? KOO B K,ROH E,YANG Y S,et al.Difference between old and young adults in contribution of β-cell function and sarcopenia in developing diabetes mellitus[J].Journal of Diabetes Investigation,2016,7(2):233-240.
[5]? 王彥永,張慶,王銘維.絕經與頸動脈粥樣硬化發生發展的關系[J].中國全科醫學,2010,13(14):1607-1608.
WANG Y Y,ZHANG Q,WANG M W.Relationship between menopause and occurrence and development of carotid atherosclerosis[J].Chinese General Practice,2010,13(14):1607-1608.
[6]? VAIDYA D,GOLDEN S H,HAQ N,et al.Association of sex hormones with carotid artery distensibility in men and postmenopausal women:multi-ethnic study of atherosclerosis[J].Hypertension,2015,65(5):1020-1025.
[7]? SEO D H,LEE Y H,SUH Y J,et al.Low muscle mass is associated with carotid atherosclerosis in patients with type 2 diabetes[J].Atherosclerosis,2020,305:19-25.
[8]? HESLOP K,ROSS C.The alcohol smoking and substance involvement screening test in an acute mental health setting[J].Australian Nursing & Midwifery Journal,2014,21(11):47.
[9]? 中華醫學會骨質疏松和骨礦鹽疾病分會.肌少癥共識[J].中華骨質疏松和骨礦鹽疾病雜志,2016,9(3):215-227.
Chinese Society of Osteoporosis and Bone Mineral Diseases.Myopenia consensus[J].Chinese Journal of Osteoporosis and Bone Mineral Research,2016,9(3):215-227.
[10]? VAN DAM-NOLEN D H K,TRUIJMAN M,VAN DER KOLK A,et al.Carotid plaque characteristics predict recurrent ischemic stroke:the Plaque At Risk(PARISK) study[J].Atherosclerosis,2022,355:29.
[11]? 王勇,王存川,朱曬紅,等.中國肥胖及2型糖尿病外科治療指南(2019版)[J].中國實用外科雜志,2019,39(4):301-306.
WANG Y,WANG C C,ZHU S H,et al.Guidelines for surgical treatment of obesity and type 2 diabetes in China(2019 edition)[J].Chinese Journal of Practical Surgery,2019,39(4):301-306.
[12]? 中國高血壓防治指南編寫組,中國高血壓聯盟,中華醫學會心血管病學分會,等.中國高血壓防治指南(2018年修訂版)[J].中國心血管雜志,2019,24(1):24-56.
Writing Group of Chinese Guidelines for the Management of Hypertension,Chinese Hypertension League,Chinese Society of Cardiology,et al.2018 Chinese guidelines for the management of hypertension[J].Chinese Journal of Cardiovascular Medicine,2019,24(1):24-56.
[13]? KNOWLTON A A,LEE A R.Estrogen and the cardiovascular system[J].Pharmacology & Therapeutics,2012,135(1):54-70.
[14]? DOS SANTOS R L,DA SILVA F B ,RIBEIRO R F J,et al.Sex hormones in the cardiovascular system[J].Hormone Molecular Biology and Clinical Investigation,2014,18(2):89-103.
[15]? CHIU T H,CHEN S C,YU H C,et al.Association between geriatric nutrition risk index and skeletal muscle mass index with bone mineral density in post-menopausal women who have undergone total thyroidectomy[J].Nutrients,2020,12(6):1683.
[16]? KO J,PARK Y M.Menopause and the loss of skeletal muscle mass in women[J].Iranian Journal of Public Health,2021,50(2):413-414.
[17]? MALTAIS M L,DESROCHES J,DIONNE I J.Changes in muscle mass and strength after menopause[J].Journal of Musculoskeletal & Neuronal Interactions,2009,9(4):186-197.
[18]? DAVISON S L,BELL R,DONATH S,et al.Androgen levels in adult females:changes with age,menopause,and oophorectomy[J].The Journal of Clinical Endocrinology & Metabolism,2005,90(7):3847-3853.
[19]? STRAUB R H.The complex role of estrogens in inflammation[J].Endocrine Reviews,2007,28(5):521-574.
[20]? AGOSTINI D,ZEPPA D S,LUCERTINI F,et al.Muscle and bone health in postmenopausal women:role of protein and vitamin D supplementation combined with exercise training[J].Nutrients,2018,10(8):1103.
[21]? DRUMMOND M J,FRY C S,GLYNN E L,et al.Rapamycin administration in humans blocks the contraction-induced increase in skeletal muscle protein synthesis[J].The Journal of Physiology,2009,587(Pt 7):1535-1546.
[22]? MOREAU K L.Modulatory influence of sex hormones on vascular aging[J].American Journal of Physiology Heart and Circulatory Physiology,2019,316(3):H522-H526.
[23]? WANG C Y,ZHANG W,WANG Y Y,et al.Novel associations between sex hormones and diabetic vascular complications in men and postmenopausal women:a cross-sectional study[J].Cardiovascular Diabetology,2019,18(1):97.
[24]? MILLER A A,DE SILVA T M,JACKMAN K A,et al.Effect of gender and sex hormones on vascular oxidative stress[J].Clinical and Experimental Pharmacology & Physiology,2007,34(10):1037-1043.
[25]? 白瑞娜,李立志.老年女性高血壓之衰老病因與病理機制[J].中西醫結合心腦血管病雜志,2015,13(14):1690-1692.
BAI R N,LI L Z.Etiology and pathological mechanism of aging in elderly women with hypertension[J].Chinese Journal of Integrative Medicine on Cardio/Cerebrovascular Disease,2015,13(14):1690-1692.
[26]? EL ASSAR M,ANGULO J,RODR?GUEZ-MA?AS L.Oxidative stress and vascular inflammation in aging[J].Free Radical Biology & Medicine,2013,65:380-401.
[27]? CLEASBY M E,JAMIESON P M,ATHERTON P J.Insulin resistance and sarcopenia:mechanistic links between common comorbidities[J].The Journal of Endocrinology,2016,229(2):R67-R81.
[28]? MORLEY J E.Hormones and sarcopenia[J].Current Pharmaceutical Design,2017,23(30):4484-4492.
[29]? KAWADA T.Insulin resistance and sarcopenia are closely related to metabolic syndrome in male and female adolescents[J].Public Health Nutrition,2016,19(8):1528.
[30]? KIM S H,KANG H W,JEONG J B,et al.Association of obesity,visceral adiposity,and sarcopenia with an increased risk of metabolic syndrome:a retrospective study[J].PLoS One,2021,16(8):e0256083.
[31]? 夏青,戈凌霞,盧亞運,等.絕經早期女性代謝肥胖與頸動脈斑塊的關聯研究[J].預防醫學,2021,33(10):1077-1080.
XIA Q,GE L X,LU Y Y,et al.Relationship between metabolic obesity phenotypes and carotid plaque in women at early stage of menopause[J].Preventive Medicine,2021,33(10):1077-1080.
(收稿日期:2023-06-16;修回日期:2024-04-08)
(本文編輯 崔曉芳)
猜你喜歡
現代經濟信息(2016年19期)2016-10-20 18:46:44
現代經濟信息(2016年19期)2016-10-20 18:12:28
現代經濟信息(2016年19期)2016-10-20 16:20:30
中國科技博覽(2016年19期)2016-10-19 13:33:22
中國科技博覽(2016年18期)2016-10-19 10:49:54
中國科技博覽(2016年18期)2016-10-19 08:16:45
中國科技博覽(2016年18期)2016-10-19 06:39:44
中國市場(2016年36期)2016-10-19 03:54:01
中國市場(2016年35期)2016-10-19 02:30:10
商(2016年27期)2016-10-17 07:09:07