阿托伐他汀對慢性阻塞性肺病合并冠心患者炎性標志物的影響
2015-03-07 12:51:43陳閃閃張福瑞張國俊
實用臨床醫藥雜志 2015年17期
關鍵詞:阿托伐他汀
陳閃閃, 白 勇, 張福瑞, 張國俊
(鄭州大學第一附屬醫院 呼吸與危重醫學一科, 河南 鄭州, 450052)
?
阿托伐他汀對慢性阻塞性肺病合并冠心患者炎性標志物的影響
陳閃閃, 白勇, 張福瑞, 張國俊
(鄭州大學第一附屬醫院 呼吸與危重醫學一科, 河南 鄭州, 450052)
摘要:目的探討阿托伐他汀對慢性阻塞性肺病合并冠心病患者炎性標志物的影響。方法收集穩定型COPD患者112例,隨機分為對照組(常規對癥治療)和阿托伐他汀治療組(常規對癥治療+阿托伐他汀)。在入院24 h內收集血液測定患者血脂、肺功能等指標;在治療6周后,測定血中總膽固醇水平、低密度脂蛋白膽固醇、纖維蛋白原、超敏C反應蛋白(hs-CRP)、TNF-α和IL-6水平。結果阿托伐他汀治療組血中總膽固醇和低密度脂蛋白膽固醇水平明顯低于對照組(P<0.01), 并且TNF-α水平和IL-6水平均明顯低于對照組(P<0.05)。但阿托伐他汀治療組用力肺活量和第1秒用力呼氣容積/用力肺活量與對照組比較無顯著差異(P>0.05)。結論阿托伐他汀不但具有降脂作用,還能降低COPD合并冠心病患者血中的炎癥標志物,可能對COPD合并冠心病患者具有有益影響。
關鍵詞:慢性阻塞性肺病; 阿托伐他汀; 炎性標志物
慢性阻塞性肺病(COPD)是一種慢性和進展的炎性肺部疾病,主要表現是不可逆轉的氣流受限。由于煙草的消費、燃料的燃燒以及老齡化,發達國家和發展中國家中人群的COPD發病率明顯增加[1]。據估計到2020年,COPD將躍居成為造成全球死亡的第3死因[2]。COPD已成為全球主要的健康問題之一。研究[2-3]已表明COPD與增加的心血管疾病風險相關,并且在心血管病人中,COPD的伴發與心血管病人增加的疾病狀態相關,包括癥狀的惡化和頻繁的入院治療。此外,心血管疾病也是導致COPD患者死亡率的一個重要原因[4]。有研究[5]報道,辛伐他汀能降低COPD病人血中C反應蛋白水平;阿托伐他汀不但具有降低心血管事件的作用,還對COPD患者具有有益影響[6]。本文探討給予穩定型COPD合并冠心病患者阿托伐他汀是否能影響血中選擇性炎性標志物的水平。
1資料與方法
1.1 研究對象
選擇2011年7月—2013年7月在本院呼吸科住院治療的穩定型COPD患者112例,患者在過去1個月沒有惡化。COPD病例的診斷均依據中華醫學會呼吸病學分會慢性阻塞性肺疾病(COPD)學組修訂的COPD診治指南的診治標準(2007年)[7]; 冠心病的診斷標準依據冠狀動脈造影。本研究的排除標準為:過去3個月使用阿托伐他汀或皮質類固醇;不穩定性心絞痛;在過去6個月發生過心肌梗死;充血性心力衰竭;炎癥性疾病;肝功能紊亂;腎衰竭;發生癌癥。本研究方案經本院醫學倫理委員會批準,研究對象均簽署知情同意書。
1.2 實驗分組
收集全部患者的一般信息、吸煙史和醫療史等。對患者進行物理檢查、呼吸功能測定、超聲心動圖和心電圖檢查。全部患者被隨機分為2組: ① 對照組,給予患者吸氧、抗感染、止咳化痰(氨溴索注射液60 mg)和平喘(多索茶堿注射液0.3 g)等常規對癥治療,但不給于阿托伐他汀治療; ② 阿托伐他汀治療組,給予患者常規對癥治療的同時,給予阿托伐他汀(輝瑞制藥有限公司,規格20 mg×7片)20 mg/d, 連續治療6周。
1.3 指標測定
在入院第1天早晨用真空采血管留取患者的血樣,在1 500 g下離心10 min, 吸取血清并儲存于-80℃冰箱中待用;實驗開始前,用奧林巴斯全自動生化儀(OLYMPUSAU-600)測定所有患者的甘油三酯、總膽固醇、高密度脂蛋白膽固醇、低密度脂蛋白膽固醇、肌酐、尿素氮和肌酸激酶。患者纖維蛋白原、超敏C反應蛋白(hs-CRP)、TNF-α和IL-6用ELISA試劑盒測定(上海百沃公司)。治療6周后對患者進行隨訪,留取血樣,并測定相關生化指標。分別在入院時和治療6周后,用肺功能測定儀測定患者第1秒用力呼氣容積(FEV1)和用力肺活量(FVC)。
2結果
阿托伐他汀治療組患者BMI水平明顯高于對照組,差異有統計學意義(P<0.05); 2組其他指標差異無統計學意義。見表1。

表1 2組研究對象基線資料比較
與對照組比較,*P<0.05。
阿托伐他汀治療組的FEV1%和FEV1/FVC比值和對照組比較無效顯著差異(P>0.05), 但阿托伐他汀治療組的總膽固醇和低密度脂蛋白膽固醇水平明顯低于對照組,差異有統計學意義(P<0.01)。見表2。阿托伐他汀治療組患者血中TNF-α水平和IL-6水平均明顯低于對照組,差異有統計學意義(P<0.05)。見表3。
在實驗進行過程中,2組病人治療6周后均未報告嚴重COPD進展事件或心血管事件;試驗未發現嚴重不良反應事件。

表2 2組患者治療6周后各項指標比較
與對照組比較,*P<0.05,**P<0.01。
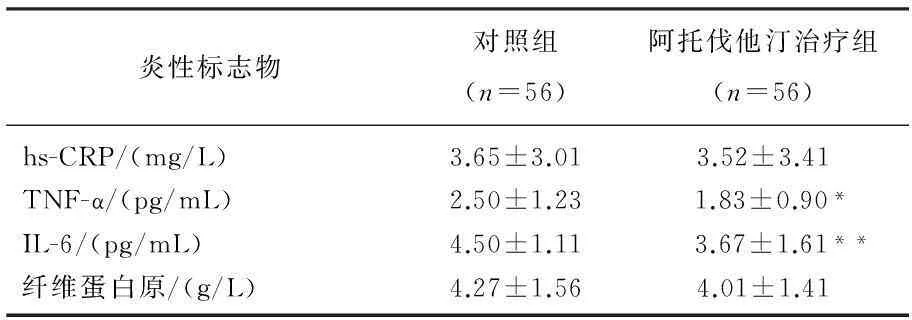
表3 2組患者治療6周后炎性標志物水平比較
與對照組比較,*P<0.05,**P<0.01。
3討論
最近的研究[8]顯示25%的心血管病患者會伴發COPD。研究[9]報道,惡化的COPD能增加患者心肌梗死和卒中的風險,并且與單純COPD患者相比, COPD合并冠心病患者顯著增加了COPD惡化的風險和疾病負擔[10]。因此,預防COPD合并冠心病患者的COPD癥狀惡化具有重要臨床意義。COPD和心血管疾病在增加炎性狀態的同時還常常伴隨著血液凝固狀態的增加。那么能穩定血小板、抑制血小板凝集和減少炎癥狀態的他汀類藥物是否對COPD合并冠心病患者炎性標志物具有影響目前尚無報道。本研究觀察了阿托伐他汀治療對COPD合并冠心病患者血中炎性標志物的影響。
本研究發現,阿托伐他汀治療雖然對COPD合并冠心病患者的FEV1%和FEV1/FVC比值沒有影響,但明顯降低了血脂水平,這與應勇等[11]在COPD患者中觀察到的結果一致。最初認為COPD主要影響肺的功能,現在認為COPD是對系統性炎癥應答的疾病,并且和慢性炎癥相關。IL-6是由支氣管上皮細胞和樹突細胞、CD8+和CD4+T細胞釋放的多效性促炎癥因子,被認為在COPD的發生中起關鍵作用[12],并且與COPD發病呈負相關[13]。Ferrari等[14]對COPD患者進行連續3年的隨訪調查發現,用IL-6評估COPD患者的系統性炎癥更持久和穩定,并且增加的IL-6水平和患者的死亡率和惡化的癥狀相關;炎性標志物CRP水平與COPD患者的癥狀惡化相關,并且系統性炎癥調節子IL-6和CRP水平在COPD患者外周血中是增加的。TNF-α是由單核巨噬細胞釋放的炎癥因子,并且 TNF-α和COPD患者的氣道炎癥及COPD的病理過程相關。本研究發現,阿托伐他汀治療降低了血中炎性標志物IL-6和TNF-α的水平,這表明應用他汀類治療COPD合并冠心病患者不但能降低血脂水平,降低心血管事件的風險;而且還能降低COPD合并冠心病患者的系統性炎癥狀態,進而降低系統性炎癥所帶來的不良臨床結局。
參考文獻
[1]Landis, Muellerova, Mannino, et al. Continuing to Confront COPD International Patient Survey: methods, COPD prevalence, and disease burden in 2012-2013 [J]. International journal of chronic obstructive pulmonary disease, 2014, 9(53): 597.
[2]Fuhrman, Delmas. Epidemiology of chronic obstructive pulmonary disease in France[J]. Revue des maladies respiratoires, 2010, 27(2): 160.
[3]Finkelstein, Cha, Scharf. Chronic obstructive pulmonary disease as an independent risk factor for cardiovascular morbidity[J]. International journal of chronic obstructive pulmonary disease, 2009, 4(32): 337.
[4]Hawkins, Huang, Pieper, et al. Chronic obstructive pulmonary disease is an independent predictor of death but not atherosclerotic events in patients with myocardial infarction: analysis of the Valsartan in Acute Myocardial Infarction Trial (VALIANT)[J]. European journal of heart failure, 2009, 11(3): 292.
[5]Kaczmarek, Sladek, Skucha, et al. The influence of simvastatin on selected inflammatory markers in patients with chronic obstructive pulmonary disease[J]. Polskie Archiwum Medycyny Wewnetrznej, 2010, 120(1/2): 11.
[6]Ishida, Kajiwara, Ishii, et al. Decrease in mortality rate of chronic obstructive pulmonary disease (COPD) with statin use: a population-based analysis in Japan[J]. The Tohoku journal of experimental medicine, 2007, 212(3): 265.
[7]慢性阻塞性肺疾病診治指南(2007年修訂版)[J]. 中華結核和呼吸雜志, 2007, (01): 8.
[8]Onishi, Yoshimoto, Hagan, et al. Prevalence of airflow limitation in outpatients with cardiovascular diseases in Japan[J]. International journal of chronic obstructive pulmonary disease, 2014, 9(563): 8.
[9]Donaldson, Hurst, Smith, et al. Increased risk of myocardial infarction and stroke following exacerbation of COPD[J]. Chest, 2010, 137(5): 1091.
[10]Dalal, Shah, Lunacsek, et al. Clinical and economic burden of patients diagnosed with COPD with comorbid cardiovascular disease[J]. Respiratory medicine, 2011, 105(10): 1516.
[11]應勇, 張敏華, 湯強. 阿托伐他汀對慢阻肺患者血漿炎癥細胞因子的影響及療效觀察[J]. 藥物流行病學雜志, 2013, (02): 57.
[12]Lamela, Vega. Immunologic aspects of chronic obstructive pulmonary disease[J]. N Engl J Med, 2009, 361(10): 1024.
[13]Bade, Khan, Srivastava, et al. Serum cytokine profiling and enrichment analysis reveal the involvement of immunological and inflammatory pathways in stable patients with chronic obstructive pulmonary disease[J]. International journal of chronic obstructive pulmonary disease, 2014, 9(23): 759.
[14]Ferrari, Tanni, Caram, et al. Three-year follow-up of Interleukin 6 and C-reactive protein in chronic obstructive pulmonary disease[J]. Respiratory research, 2013, 14(24): 231.
Influence of atorvastatin on inflammatory markers in patients with chronic obstructive pulmonary disease and coronary heart disease
CHEN Shanshan, BAI Yong, ZHANG Furui, ZHANG Guojun
(DepartmentofRespiratoryandCriticalCareMedicine,TheFirstAffiliatedHospitalofZhengzhouUniversity,Zhengzhou,Henan, 450052)
ABSTRACT:ObjectiveTo explore the influence of atorvastatin on inflammatory markers in patients with chronic obstructive pulmonary disease (COPD) and coronary heart disease (CVD). MethodsA total of 112 patients with COPD and CVD were collected. All the patients were randomly divided into control group (symptomatic treatment) and atorvastatin group (symptomatic treatment + atorvastatin). Blood samples were collected within 24 hours after hospital admission in order to detect plasma lipid (including TG, TC, HDL and LDL) and pulmonary respiration parameters. After 6 weeks of treatment, the TG, LDL, fibrinogen, hs-CRP, TNF-α and IL-6 in serum were detected. ResultsThe TG and LDL levels in serum of the atorvastatin group were significantly lower than those of the control group (P<0.01), and the TNF-α and IL-6 levels in serum of the atorvastatin group were significantly lower than those of the control group (P<0.05 orP<0.01). There was no significant differences of FEV1 and FEV1/FVC between two groups (P>0.05). ConclusionAtorvastatin can not only decrease the level of serum lipid, but also decrease inflammatory markers in blood of patients with COPD and CVD. Atorvastatin treatment may play a beneficial effect on patients with COPD and CVD.
KEYWORDS:chronic obstructive pulmonary disease; atorvastatin; inflammatory markers
通信作者:張國俊
基金項目:河南省醫學科技攻關計劃重點項目(201302005)
收稿日期:2015-03-20
中圖分類號:R 441.8
文獻標志碼:A
文章編號:1672-2353(2015)17-005-03
DOI:10.7619/jcmp.201517002
猜你喜歡
中國現代醫生(2016年27期)2016-12-21 16:42:20
華夏醫學(2016年4期)2016-12-12 00:23:03
中國實用醫藥(2016年28期)2016-12-07 08:00:24
中國實用醫藥(2016年28期)2016-12-07 07:49:26
中國實用醫藥(2016年28期)2016-12-07 07:22:22
中國實用醫藥(2016年27期)2016-11-30 12:53:52
中外醫學研究(2016年26期)2016-11-30 04:48:45
中外醫學研究(2016年28期)2016-11-28 07:03:50
今日健康(2016年12期)2016-11-17 12:06:09
今日健康(2016年12期)2016-11-17 11:46:28
