丁酸鈉聯合順鉑對卵巢透明細胞癌ES-2細胞活性及增殖的影響
2016-01-20 13:54:00蘇強馬妮娜李琴俞靜張晨光首都醫科大學附屬北京友誼醫院北京100050
山東醫藥 2015年32期
關鍵詞:順鉑
蘇強,馬妮娜,李琴,俞靜,張晨光(首都醫科大學附屬北京友誼醫院,北京100050)
丁酸鈉聯合順鉑對卵巢透明細胞癌ES-2細胞活性及增殖的影響
蘇強,馬妮娜,李琴,俞靜,張晨光
(首都醫科大學附屬北京友誼醫院,北京100050)
摘要:目的觀察丁酸鈉聯合順鉑對卵巢透明細胞癌ES-2細胞活性及增殖的影響。方法將對數生長期的卵巢透明細胞癌ES-2細胞隨機分為觀察組和對照組。觀察組分別加入1、2、4、6 mmol/L的丁酸鈉和5 μg/mL順鉑,對照組分別加入與觀察組相同濃度的丁酸鈉。采用MMT法檢測兩組細胞活性,Western blotting法檢測兩組凋亡蛋白( c-PAPP、c-Caspase-3)和增殖蛋白( ERK、p-ERK)相對表達量。結果觀察組加入1、2、4、6 mmol/L丁酸鈉和順鉑細胞活性分別為51%±3%、39%±2%、22%±2%、11%±1%,多組間及組內兩兩比較,P均<0.05;對照組加入1、2、4、6 mmol/L丁酸鈉細胞活性分別為88%±4%、76%±3%、69%±2%、54%±2%,多組間及組內兩兩比較,P均<0.05;兩組加入相同濃度丁酸鈉細胞活性比較,P均<0.05。隨著丁酸鈉濃度增加,兩組凋亡蛋白c-PAPP、c-Caspase-3相對表達量逐漸升高,增殖蛋白ERK、p-ERK相對表達量逐漸降低。與對照組同濃度丁酸鈉比較,觀察組1、2、4、6 mmol/L丁酸鈉和順鉑c-PAPP、c-Caspase-3蛋白表達均升高,1、6 mmol/L丁酸鈉和順鉑ERK、p-ERK蛋白表達均降低;兩組比較,P均<0.05。結論丁酸鈉聯合順鉑可降低卵巢透明細胞癌ES-2細胞活性,抑制其增殖、促進其凋亡;丁酸鈉濃度越高,上述作用越明顯。
關鍵詞:卵巢腫瘤;卵巢透明細胞癌;丁酸鈉;順鉑;細胞活性;增殖蛋白;凋亡蛋白
Effect of sodium butyrate combined with cisplatin on cell viability and proliferation of ovarian clear cell carcinoma ES-2 cells
SU Qiang,MA Ni-na,LI Qin,YU Jing,ZHANG Chen-guang
( Beijing Friendship Hospital Affiliated to Capital Medical University,Beijing 100050,China)
Abstract:Objective To observe the effect of sodium butyrate combined with cisplatin on cell viability and proliferation of ovarian clear cell carcinoma ES-2 cells.Methods The ovarian clear cell carcinoma ES-2 cells in the logarithmic phase were randomly divided into the observation groups and control groups.The observation groups were added 1,2,4 and 6 mmol/L sodium butyrate ( NaB) and 5 μg/mL cisplatin.The control groups were added the same concentrations of NaB.The cell activities were detected by MMT,and the relative expression levels of c-PAPP,c-Caspase-3,ERK and p-ERK were detected by Western blotting.Results The cell viabilities of the observation groups which were treated with 1,2,4,6 mmol/L NaB and 5 μg/mL cisplatin were 51%±3%,39%±2%,22%±2% and 11%±1%,respectively; and significant difference was found between groups ( all P<0.05).The cell viabilities of the control groups were 88%± 4%,76%±3%,69%±2% and 54%±2%,respectively; and significant difference was found between groups ( all P<0.05).Meanwhile,significant difference was found in the cell viability between the two groups which were added with the same concentrations of NaB ( all P<0.05).With the increased concentrations of NaB,the relative expression levels of c-PAPP and c-Caspase-3 in the two kinds of groups were gradually increased,and the levels of ERK and p-ERK were significantly decreased.Compared with the control groups,the relative expression levels of c-PAPP and c-Caspase-3 in the observation groups which were added 1,2,4 and 6 mmol/L NaB and 5 μg/mL cisplatin were all increased and the levels of ERK and P-ERK were decreased in the observation groups which were added 1 and 6 mmol/L NaB and 5 μg/mL cisplatin.Significant difference was found between the two kinds of groups ( all P<0.05).Conclusion NaB combined with cispla-
tin may decrease the cell viability of ovarian clear cell carcinoma ES-2 cells,inhibit the proliferation and promote the apoptosis.The effect can be stronger with the higher concentrations of NaB.
Key words:ovarian neoplasms; ovarian clear cell carcinoma; sodium butyrate; cisplatin; cell viability; proliferin; apoptin
卵巢透明細胞癌發病率呈逐漸升高趨勢,其術后復發率高,對鉑類化療藥物不敏感;化療耐藥是影響患者預后的主要因素;增強患者的順鉑化療敏感性是近年來國內外研究的熱點。丁酸鈉( NaB)是組蛋白去乙酰化酶抑制劑,可通過抑制組蛋白去乙酰化酶松弛染色質結構,促進腫瘤細胞凋亡,并抑制其生長[1],但其是否可增加卵巢透明細胞癌患者對順鉑化療的敏感性鮮見報道。2014年8~12月,我們觀察了NaB聯合5 μg/mL順鉑對卵巢透明細胞癌ES-2細胞活性及增殖的影響。
1 材料與方法
1.1材料人卵巢透明細胞癌ES-2細胞由首都醫科大學附屬遺傳學實驗室傳代培養。順鉑購自山東齊魯制藥有限公司,NaB、ERK、P-ERK、Caspase-3、PARP一抗、二抗均購自美國Sigma-Aldrich公司。酶聯免疫檢測儀購于美國BioTek公司,全套聚丙烯酰胺電泳設備購于美國Bio-Rad公司,自動洗片機購于美國ALL PRO公司。
1.2細胞培養及分組處理將人卵巢透明細胞癌ES-2細胞置于含10% FBS及青鏈霉素的RPMI-1640培養基中,于37℃、5% CO2的無菌培養箱中培養,3 d傳代1次。將對數生長期的人卵巢癌ES-2細胞隨機分為觀察組和對照組,按每孔1×104個接種至96孔板中,每孔設3個復孔。加入100 μL的培養液后,觀察組分別加入1、2、4、6 mmol/L的NaB和5 μg/mL順鉑,對照組分別加入1、2、4、6 mmol/L的NaB。
1.3相關指標觀察
1.3.1細胞活性采用MTT法。兩組置于37℃、5% CO2的無菌培養箱中培養72 h,同時以加入二甲基亞砜( DMSO)的細胞作為對照。吸棄培養基后PBS沖洗3次,加入完全培養基100 μL。各孔加入MTT溶液10 μL,37℃孵育2 h,脫色搖床振蕩10 min。于酶標儀上測定波長570 nm處各孔吸光度( OD值),細胞活性= ( OD細胞-OD對照)/OD對照×100%。
1.3.2細胞凋亡蛋白( c-PAPP、c-Caspase-3)及增殖蛋白( ERK、p-ERK)表達采用Western blotting法。收集兩組培養72 h后的細胞,接種至培養瓶內培養,棄培養液后用冰冷PBS沖洗2次。細胞刮刀收集細胞,裂解液重懸細胞,12 000 r/min離心30 min,取上清,于-80℃保存。采用考馬斯亮藍法測定蛋白濃度,聚丙烯酸胺凝膠電泳,電轉移至硝酸纖維素膜上,5%脫脂奶粉封閉。分別加入一抗室溫孵育2 h,加入二抗室溫孵育45 min。以Odyssey熒光掃描儀掃描顯影,Quantity one軟件計算灰度比值以β-actin為內參,采用Image J軟件計算凋亡蛋白( c-PAPP、c-Caspase-3)及增殖蛋白( ERK、p-ERK)的相對表達量。
1.4統計學方法采用SPSS13.0統計軟件。計量資料以珋x±s表示,多組間比較采用秩和檢驗,兩組間比較采用t檢驗。P<0.05為差異有統計學意義。
2 結果
2.1兩組細胞活性比較觀察組加入1、2、4、6 mmol/L NaB和順鉑的細胞活性分別為51%±3% 39%±2%、22%±2%、11%±1%,多組間及組內兩兩比較,P均<0.05;對照組加入1、2、4、6 mmol/L NaB細胞活性分別為88%±4%、76%±3%、69% ±2%、54%±2%,多組間及組內兩兩比較,P均<0.05;兩組相同濃度NaB細胞活性比較,P均<0.05。
2.2兩組凋亡蛋白及增殖蛋白表達比較隨著NaB濃度的增加,兩組凋亡蛋白c-PAPP、c-Caspase 3相對表達量逐漸升高,增殖蛋白ERK、p-ERK相對表達量逐漸降低。兩組凋亡蛋白及增殖蛋白表達比較見表1。
3 討論
卵巢透明細胞癌臨床少見,惡性程度極高,占卵巢惡性腫瘤的5%~13%[2]。鉑類是臨床上治療卵巢惡性腫瘤最常用的化療藥物,順鉑主要作用于DNA鏈間及鏈內絞鏈,形成DDP-DNA復合物而干擾DNA復制;或與核蛋白及胞漿蛋白結合,抑制腫瘤細胞生長而導致其死亡。但卵巢透明細胞癌對于鉑類化療不敏感[3]。研究表明,卵巢上皮性癌的化療有效率(含鉑類)為73%~81%,而卵巢透明細胞癌的一線化療有效率(含鉑類)為11%~27%[4~6];對于復發的卵巢透明細胞癌,二線化療有效率(含鉑類)<10%[7,8]。因此,如何增強卵巢透明細胞癌對于順鉑的化療敏感性成為國內外研究的熱點。
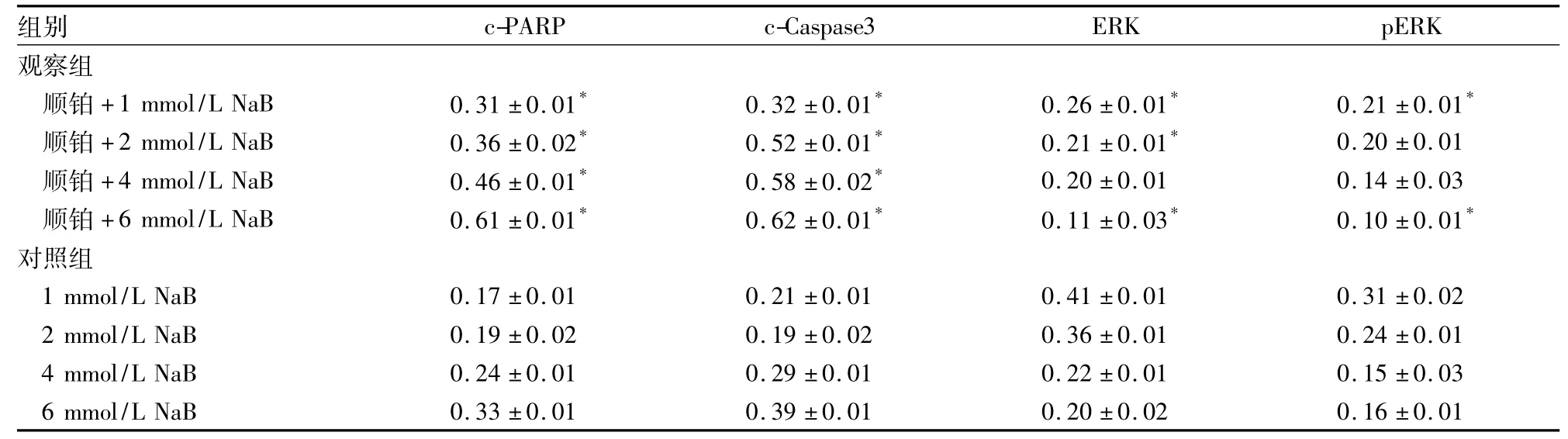
表1 兩組凋亡蛋白c-PAPP、c-Caspase-3及增殖蛋白ERK、p-ERK表達比較(相對表達量,珔x±s)
研究表明,腫瘤發生與組蛋白N端賴氨酸殘基的乙酰化和去乙酰化過程失衡密切相關,其中組蛋白乙酰轉移酶和組蛋白去乙酰基酶( HDAC)共同控制著組蛋白的乙酰化水平,兩者的動態平衡控制著染色質結構和基因表達,其動態失衡與多種腫瘤發生有關[9,10]。組蛋白去乙酰基酶抑制劑( HDACI)可通過促進組蛋白的乙酰化以及促進非組蛋白底物的乙酰化發揮抗癌活性;其基因轉錄異常可阻滯細胞周期,抑制DNA修復,從而誘導細胞凋亡[11]。有研究表明,HDACI與一些傳統化療藥物共同應用可能會降低化療藥物介導的腫瘤細胞凋亡的閾值,具有協同抗腫瘤作用[12,13]。NaB屬于HDACI的短鏈脂肪酸鹽,可通過抑制HDAC松弛染色質結構,促進抑癌基因表達,具有抑制腫瘤細胞生長的作用[14]。
前期研究顯示,5 μg/mL的順鉑作用于卵巢透明細胞癌ES-2細胞后,其細胞活度約為50%,因此本實驗選擇此濃度進行研究。本研究結果顯示,與對照組加入相同濃度NaB比較,觀察組細胞活性和凋亡蛋白c-PAPP、c-Caspase-3相對表達量均顯著升高,增殖蛋白ERK、p-ERK相對表達量均顯著降低;說明NaB聯合順鉑可降低卵巢透明細胞癌ES-2細胞活性,并抑制其增殖、促進其凋亡;且觀察組上述指標變化隨NaB濃度的增加而變化更明顯,說明其具有一定的濃度依賴性。本實驗屬于細胞水平的初步研究,NaB聯合順鉑對卵巢透明細胞癌ES-2細胞增殖的抑制作用及其機制仍需要進一步的動物、分子甚至臨床水平的深入研究。
參考文獻:
[1]Minucci S,Pelicci PG.Histone deacetylase inhibitors and the promise of epigenetic and more treatments for cancer[J].Nat Rev Cancer,2006,6( 1) :38-51.
[2]修敏,郭玲,劉絲蓀.卵巢透明細胞癌發病與耐藥分子機制的研究進展[J].腫瘤,2014,34( 10) : 963-968.
[3]Jemal A,Siegel R,Xu J,et al.Cancer statistics[J].CA Cancer J Clin,2010,60( 5) : 277-300.
[4]Sugiyama T,Yakushiji M,Nishida T,et al.Irinotecan ( CPT-11) combined with cisplatin in patients with refractory or recurrent o varian cancer[J].Cancer Lett,1998,128( 2) : 211-218.
[5]Ho CM,Huang YJ,Chen TC,et al.Pure-type clear cell carcino ma of the ovary as a distinct histological type and improved surviva in patients treated with paclitaxel-platinum-based chemotherapy in pure-type advanced disease[J].Gynecol Oncol,2004,94( 1) : 197-203.
[6]Utsunomiya H,Akahira J,Tanno S,et al.Paclitaxel-platinum combination chemotherapy for advanced or recurrent ovarian clea cell adenocarcinoma: a multicenter trial[J].Int J Gynecol Canc er,2006,16( 1) : 52-56.
[7]Takano M,Kikuchi Y,Kudoh K,et al.Weekly administration o temsirolimus for heavily pretreated patients with clear cell carcino ma of the ovary: a report of six cases[J].Int J Clin Oncol,2011 16( 5) : 605-609.
[8]Takano M,Kikuchi Y,Yaegashi N,et al.Clear cell carcinoma o the ovary: aretrospective multicentre experience of 254 patient with complete surgical staging[J].Br J Cancer,2006,94( 10) : 1369-1374.
[9]Kristensen LS,Nielsen HM,Hansen LL.Epigenetics and cance treatment[J].Eur J Pharmacol,2009,625( 1) : 131-142.
[10]崔路佳,高善玲,裴鳳華.丁酸鈉抗腫瘤作用的新進展[J].世界華人消化雜志,2015,13( 14) : 1744-1746.
[11]Lakshmaiah KC,Jacob LA,Aparna S,et al.Epigenetic therapy o cancer with histone deacetylase inhibitors[J].J cancer Res Ther 2014,10( 3) : 469-478.
[12]Arnold NB,Arkus N,Gunn J,et al.The histone deacetylase in hibitor suberoylanilidehydroxamic acid induces growth inhibition and enhances gemcitabine-induced cell death in pancreatic cance [J].Clin Cancer Res,2007,13( 1) : 18-26.
[13]Dowdy SC,Jiang S,Zhou XC,et al.Histonedeacetylase inhibitor and paclitaxel cause synergistic effects on poptosis and microtubule stabilization in papillary serous endometrial cancer cells[J].Mo Cancer Ther,2006,5( 11) : 2767-2776.
[14]董梅,胡興勝,陳閃閃,等.組蛋白去乙酰化酶抑制劑在腫瘤治療領域的進展[J].中華腫瘤學雜志,2013,35( 7) : 481-485.
收稿日期:( 2015-06-13)
通信作者簡介:張晨光( 1980-),男,高級講師,研究方向為實體惡性腫瘤的基礎。E-mail: chzhang@ ccmu.edu.cn
作者簡介:第一蘇強( 1978-),男,主治醫師,研究方向為實體惡性腫瘤的臨床與基礎。E-mail: BJSQ1978@163.com
基金項目:國家自然科學基金青年基金資助項目( 81201816) ;首都醫科大學臨床基礎合作研究基金資助項目( 15JL33) ;首都醫科大學附屬北京友誼醫院院啟動基金資助項目( yyqdkt2014-12)。
文章編號:1002-266X( 2015) 32-0017-03
文獻標志碼:A
中圖分類號:R737.31
doi:10.3969/j.issn.1002-266X.2015.32.006
猜你喜歡
現代養生·下半月(2016年5期)2017-01-09 10:12:30
中國當代醫藥(2016年30期)2017-01-07 00:55:28
中國當代醫藥(2016年30期)2017-01-07 00:49:32
中國實用醫藥(2016年30期)2016-12-28 22:59:47
中國當代醫藥(2016年28期)2016-12-20 18:12:21
中國醫藥導報(2016年25期)2016-11-30 07:20:06
中外醫學研究(2016年28期)2016-11-28 07:12:34
中國實用醫藥(2016年26期)2016-11-07 13:49:05
中國實用醫藥(2016年24期)2016-10-17 05:10:07
中國實用醫藥(2016年24期)2016-10-17 04:52:27