178例梗阻性無精子癥危險因素及臨床特征分析
2016-11-26 00:34:46王巖斌洪鍇唐文豪田雨趙連明毛加明劉德風姜輝
中國性科學
2016年9期
王巖斌 洪鍇 唐文豪 田雨 趙連明 毛加明 劉德風 姜輝
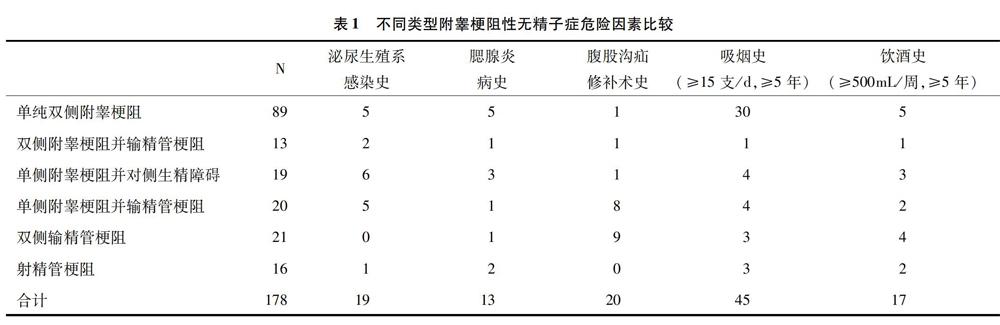
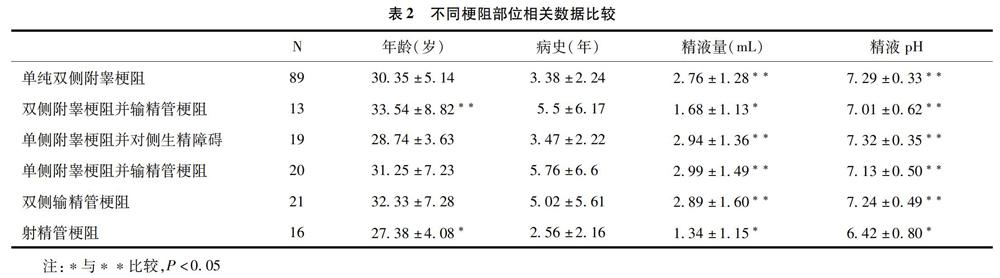
【摘要】目的:探討梗阻性無精子癥發病危險因素及臨床特點。方法:回顧性分析2014年1月至2015年12月期間收治的178例梗阻性無精子癥手術患者的臨床資料,包括既往病史、體格檢查、精液分析等,所有患者均經手術確診。結果:178例梗阻性無精子癥患者中,以附睪梗阻最為常見,共141例(79.2%),其中單純雙側附睪管梗阻89例(50%);雙側輸精管梗阻21例(11.8%);射精管梗阻16例(8.9%)。在5個常見危險因素中,有長期吸煙史者45例,與其他因素比較有顯著差異(P<0.05);輸精管梗阻的患者中既往有腹股溝疝修補術史者明顯多于其它類型的梗阻(P<0.05)。精液量與精液pH值的比較中,射精管梗阻患者較其它各組均低(P<0.05)。結論:梗阻性無精子癥中附睪梗阻最為常見;長期大量吸煙可能是梗阻性無精子癥危險因素之一;精液量及精液pH值可作為射精管梗阻性無精子癥的重要指標之一。
【關鍵詞】梗阻性無精癥;危險因素;臨床特征
【Abstract】Objectives: To investigate the risk factors and clinical features of obstructive azoospermia (OA). Methods:The records of 178 cases with OA from January 2014 to December 2015 were retrospectively studied. The clinical data and risk factors were compared. All cases were confirmed by the surgical operation. Results:Among the 178 cases, the most common type was epididymal obstruction azoospermia (141 cases, 79.2%); bilateral vas deferens obstruction was 21 cases (11.8%); ejaculatory duct obstruction was 16 cases (8.9%). Among the 5 common risk factors, 45 cases had a history of long-term smoking, with a significantly higher incidence than others (P<0.05), and there was a significantly higher incidence of a history of inguinal hernia repair for bilateral vas deferens obstruction group versus other groups (P<0.05). Both seminal volume and seminal PH of ejaculatory duct obstruction azoospermia was lower the other groups (P<0.05). Conclusion: The most common type of OA is epididymal obstruction azoospermia and long-term smoking is probably one of the risk factors of OA. Both seminal volume and seminal PH are important to the diagnosis of ejaculatory duct obstruction azoospermia.
【Key words】Abstructive azoospermia; Risk factors; Clinical features
【中圖分類號】R698+.2【文獻標志碼】A
國內資料顯示,無精癥(Azoospermia)在男性不育癥中占9.16%[1]。根據其病因,臨床中分為梗阻性無精癥(obstructive azoospermia OA)與非梗阻性無精癥(non-obstructive azoospermia, NOA)。OA約占無精癥的20%~50%[2,3]。手術是OA最主要的治療手段,對梗阻部位的準確判斷是治療的關鍵。我們通過對手術治療病例進行了回顧性研究,現總結如下。
1資料與方法
1.1一般資料
回顧性分析本院2014年1月至2015年12月收治的經手術確診的178例梗阻性無精子癥患者資料,年齡20~56歲,平均(30.37±5.90)歲。病史1~27年,平均(3.77±3.72)年。既往有生育史22例。所有病例術前均經過我院生殖醫學中心至少2次或以上精液常規分析,并將精液經離心沉渣后高倍鏡檢確診為無精子癥(精液檢查采用WHO第4版標準[4])。
1.2方法
采用我院常規手術方法[5]:患者仰臥位,氣管內插管全身麻醉。消毒、鋪巾后留置F14Foley氣囊尿管。取雙側陰囊縱切口,逐層切開皮膚、肉膜、睪丸鞘膜層,暴露睪丸、附睪,觀察睪丸和附睪形態,觸診輸精管。……
登錄APP查看全文
猜你喜歡
上海醫藥(2016年23期)2016-12-22 12:37:08
中國現代醫生(2016年27期)2016-12-21 16:21:19
中國實用醫藥(2016年28期)2016-12-07 08:59:38
今日健康(2016年12期)2016-11-17 14:41:50
今日健康(2016年12期)2016-11-17 13:12:34
今日健康(2016年12期)2016-11-17 12:29:29
科技資訊(2016年19期)2016-11-15 10:33:36
中國實用醫藥(2016年26期)2016-11-07 11:05:00
中國實用醫藥(2016年24期)2016-10-17 05:32:48
中國實用醫藥(2016年17期)2016-07-26 22:34:56
